

A Pilot Study Identifying Brain-Targeting Adaptive Immunity in Pediatric Extracorporeal Membrane Oxygenation Patients With Acquired Brain Injury
- PMID: 30640221
- PMCID: PMC6377324
- DOI: 10.1097/CCM.0000000000003621
A Pilot Study Identifying Brain-Targeting Adaptive Immunity in Pediatric Extracorporeal Membrane Oxygenation Patients With Acquired Brain Injury
Abstract
Objectives: Extracorporeal membrane oxygenation provides short-term cardiopulmonary life support, but is associated with peripheral innate inflammation, disruptions in cerebral autoregulation, and acquired brain injury. We tested the hypothesis that extracorporeal membrane oxygenation also induces CNS-directed adaptive immune responses which may exacerbate extracorporeal membrane oxygenation-associated brain injury.
Design: A single center prospective observational study.
Setting: Pediatric and cardiac ICUs at a single tertiary care, academic center.
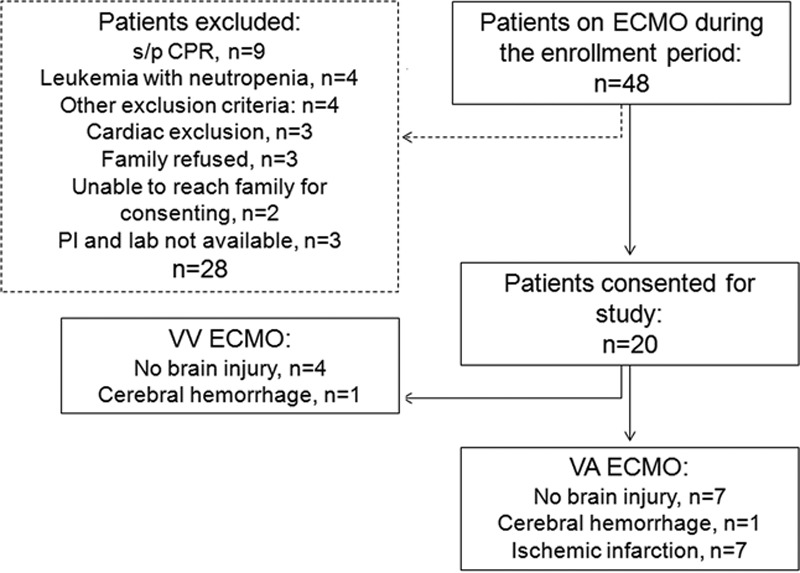
Patients: Twenty pediatric extracorporeal membrane oxygenation patients (0-14 yr; 13 females, 7 males) and five nonextracorporeal membrane oxygenation Pediatric Logistic Organ Dysfunction score matched patients INTERVENTIONS:: None.
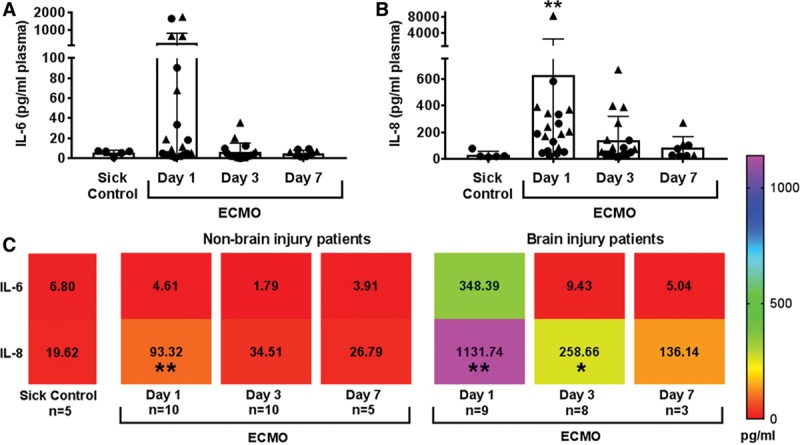
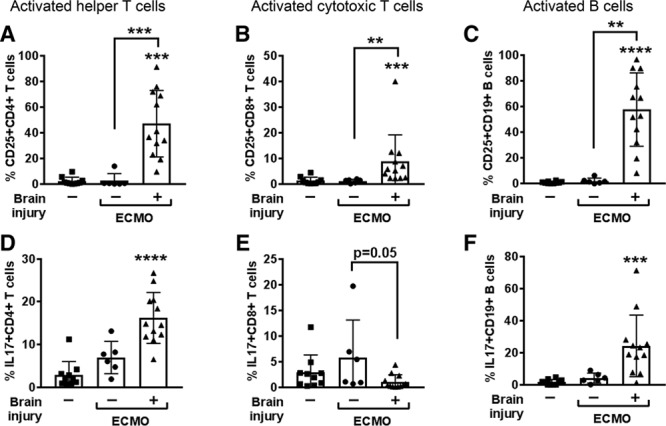
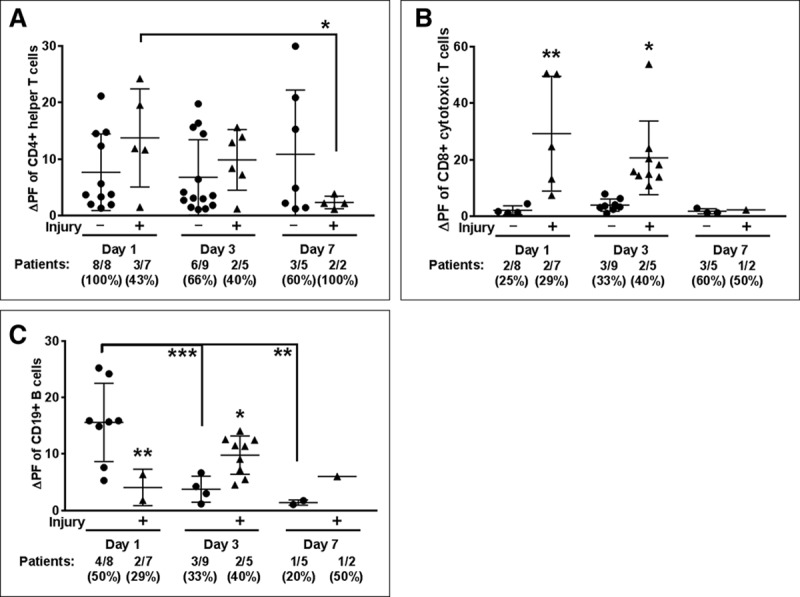
Measurements and main results: Venous blood samples were collected from the extracorporeal membrane oxygenation circuit at day 1 (10-23 hr), day 3, and day 7 of extracorporeal membrane oxygenation. Flow cytometry quantified circulating innate and adaptive immune cells, and CNS-directed autoreactivity was detected using an in vitro recall response assay. Disruption of cerebral autoregulation was determined using continuous bedside near-infrared spectroscopy and acquired brain injury confirmed by MRI. Extracorporeal membrane oxygenation patients with acquired brain injury (n = 9) presented with a 10-fold increase in interleukin-8 over extracorporeal membrane oxygenation patients without brain injury (p < 0.01). Furthermore, brain injury within extracorporeal membrane oxygenation patients potentiated an inflammatory phenotype in adaptive immune cells and selective autoreactivity to brain peptides in circulating B cell and cytotoxic T cell populations. Correlation analysis revealed a significant relationship between adaptive immune responses of extracorporeal membrane oxygenation patients with acquired brain injury and loss of cerebral autoregulation.
Conclusions: We show that pediatric extracorporeal membrane oxygenation patients with acquired brain injury exhibit an induction of pro-inflammatory cell signaling, a robust activation of adaptive immune cells, and CNS-targeting adaptive immune responses. As these patients experience developmental delays for years after extracorporeal membrane oxygenation, it is critical to identify and characterize adaptive immune cell mechanisms that target the developing CNS.
Conflict of interest statement
Drs. Ortega’s, Pandiyan’s, Windsor’s, and Stowe’s institutions received funding from Extracorporeal Life Support Organization and National Center for Advancing Translational Sciences of the National Institutes of Health (NIH) under award number UL1TR001105. Drs. Ortega, Pandiyan, Windsor, Torres, Raman, and Stowe received support for article research from the NIH. Dr. Tian’s institution received funding from the American Heart Association, and he disclosed work for hire. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Robinson S, Peek G. The role of ECMO in neonatal & paediatric patients - ScienceDirect. Paediatr Child Health 2015; 25:222–227.
-
- Madderom MJ, Reuser JJ, Utens EM, et al. Neurodevelopmental, educational and behavioral outcome at 8 years after neonatal ECMO: A nationwide multicenter study. Intensive Care Med 2013; 39:1584–1593. - PubMed
-
- Brown KL, MacLaren G, Marino BS. Looking beyond survival rates: Neurological outcomes after extracorporeal life support. Intensive Care Med 2013; 39:1870–1872. - PubMed
-
- Malfertheiner MV, Philipp A, Lubnow M, et al. Hemostatic changes during extracorporeal membrane oxygenation: A prospective randomized clinical trial comparing three different extracorporeal membrane oxygenation systems. Crit Care Med 2016; 44:747–754. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
