

Follow-up study of high-dose praziquantel therapy for cerebral sparganosis
- PMID: 30640909
- PMCID: PMC6331082
- DOI: 10.1371/journal.pntd.0007018
Follow-up study of high-dose praziquantel therapy for cerebral sparganosis
Abstract
Background: Cerebral sparganosis is the most serious complication of human sparganosis. Currently, there is no standard for the treatment of inoperable patients. Conventional-dose praziquantel therapy is the most reported treatment. However, the therapeutic outcomes are not very effective. High-dose praziquantel therapy is a useful therapeutic choice for many parasitic diseases that is well tolerated by patients, but it has not been sufficiently evaluated for cerebral sparganosis. This study aims to observe the prognoses following high-dose praziquantel therapy in inoperable patients and the roles of MRI and peripheral eosinophil absolute counts during follow-up.
Methodology: Baseline and follow-up epidemiological, clinical, radiological and therapeutic data related to 10 inoperable patients with cerebral sparganosis that were treated with repeated courses of high-dose praziquantel therapy, with each course consisting of 25 mg/kg thrice daily for 10 days were assessed, followed by analyses of the prognoses, MRI findings and peripheral eosinophil absolute counts.
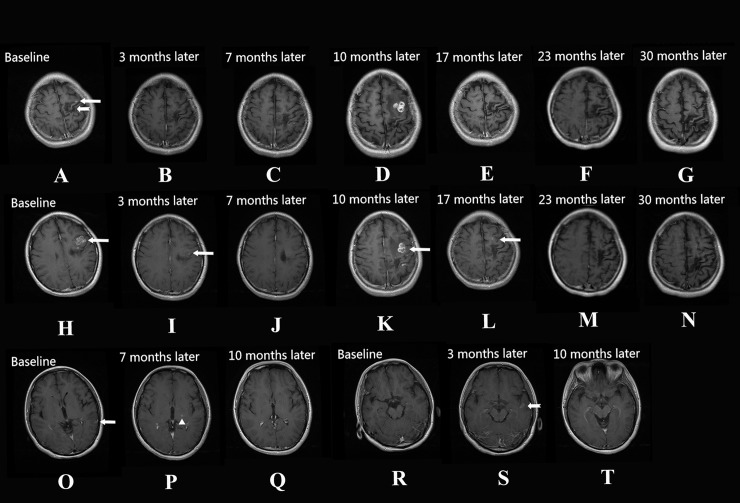
Principal findings: Baseline clinical data: the clinical symptoms recorded included seizures, hemiparesis, headache, vomiting and altered mental status. Peripheral blood eosinophilia was found in 3 patients. The baseline radiological findings were as follows. Motile lesions were observed in 10 patients, including aggregated ring-like enhancements, tunnel signs, serpiginous and irregular enhancements. Nine of the 10 patients had varying degrees of white matter degeneration, cortical atrophy and ipsilateral ventricle dilation. The follow-up clinical data were as follows. Clinical symptom relief was found in 8 patients, symptoms were eliminated in 1 patient, and symptoms showed no change from baseline in 1 patient. Peripheral blood eosinophilia was found in 2 patients. The follow-up radiological findings were as follows. Motile lesions that were transformed into stable, chronic lesions were found in 8 patients, and motile lesions that were eliminated completely were found in 2 patients.
Conclusions: High-dose praziquantel therapy for cerebral sparganosis is effective. The radiological outcomes of motile lesions are an important indicator during the treatment process, especially during follow-ups after clinical symptoms have improved. Peripheral eosinophil absolute counts cannot be used as an effective prognostic indicator.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



Similar articles
-
Cerebral sparganosis presenting with atypical postcontrast magnetic resonance imaging findings: a case report and literature review.BMC Infect Dis. 2019 Aug 27;19(1):748. doi: 10.1186/s12879-019-4396-2. BMC Infect Dis. 2019. PMID: 31455261 Free PMC article. Review.
-
Efficacy comparison between long-term high-dose praziquantel and surgical therapy for cerebral sparganosis: A multicenter retrospective cohort study.PLoS Negl Trop Dis. 2018 Oct 22;12(10):e0006918. doi: 10.1371/journal.pntd.0006918. eCollection 2018 Oct. PLoS Negl Trop Dis. 2018. PMID: 30346956 Free PMC article.
-
Cerebral sparganosis in mainland Chinese patients.J Clin Neurosci. 2013 Nov;20(11):1514-9. doi: 10.1016/j.jocn.2012.12.018. Epub 2013 Jul 30. J Clin Neurosci. 2013. PMID: 23911107
-
Sparganosis presenting as pericardial effusion and lung lesions.Intern Med. 2015;54(9):1135-9. doi: 10.2169/internalmedicine.54.3478. Epub 2015 May 1. Intern Med. 2015. PMID: 25948364
-
Clinical Features of Pulmonary Sparganosis.Am J Med Sci. 2015 Dec;350(6):436-41. doi: 10.1097/MAJ.0000000000000578. Am J Med Sci. 2015. PMID: 26465081 Review.
Cited by
-
Recent update on cerebral sparganosis: A bibliometric analysis and scientific mapping.Narra J. 2024 Aug;4(2):e982. doi: 10.52225/narra.v4i2.982. Epub 2024 Aug 15. Narra J. 2024. PMID: 39280299 Free PMC article.
-
Cerebral sparganosis presenting with atypical postcontrast magnetic resonance imaging findings: a case report and literature review.BMC Infect Dis. 2019 Aug 27;19(1):748. doi: 10.1186/s12879-019-4396-2. BMC Infect Dis. 2019. PMID: 31455261 Free PMC article. Review.
-
Proteomic and Immunological Identification of Diagnostic Antigens from Spirometra erinaceieuropaei Plerocercoid.Korean J Parasitol. 2021 Dec;59(6):615-623. doi: 10.3347/kjp.2021.59.6.615. Epub 2021 Dec 22. Korean J Parasitol. 2021. PMID: 34974668 Free PMC article.
-
Cerebral sparganosis in a child with corpus callosum invasion: a case report.BMC Infect Dis. 2023 May 25;23(1):350. doi: 10.1186/s12879-023-08322-9. BMC Infect Dis. 2023. PMID: 37231358 Free PMC article.
-
Pulmonary Sparganosis: Tunnel Sign and Migrating Sign on Computed Tomography.Intern Med. 2021 Feb 15;60(4):601-604. doi: 10.2169/internalmedicine.5304-20. Epub 2020 Sep 30. Intern Med. 2021. PMID: 32999230 Free PMC article.
References
-
- Yamashita K, Akimura T, Kawano K, et al. Cerebral sparganosis mansoni. Report of two cases. Surg Neurol.1990,33(2):28–34. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
