

18F-Fluoride Signal Amplification Identifies Microcalcifications Associated With Atherosclerotic Plaque Instability in Positron Emission Tomography/Computed Tomography Images
- PMID: 30642216
- PMCID: PMC6338081
- DOI: 10.1161/CIRCIMAGING.118.007835
18F-Fluoride Signal Amplification Identifies Microcalcifications Associated With Atherosclerotic Plaque Instability in Positron Emission Tomography/Computed Tomography Images
Abstract
Background: Microcalcifications in atherosclerotic plaques are destabilizing, predict adverse cardiovascular events, and are associated with increased morbidity and mortality.18F-fluoride positron emission tomography (PET)/computed tomography (CT) imaging has demonstrated promise as a useful clinical diagnostic tool in identifying high-risk plaques; however, there is confusion as to the underlying mechanism of signal amplification seen in PET-positive, CT-negative image regions. This study tested the hypothesis that 18F-fluoride PET/CT can identify early microcalcifications.
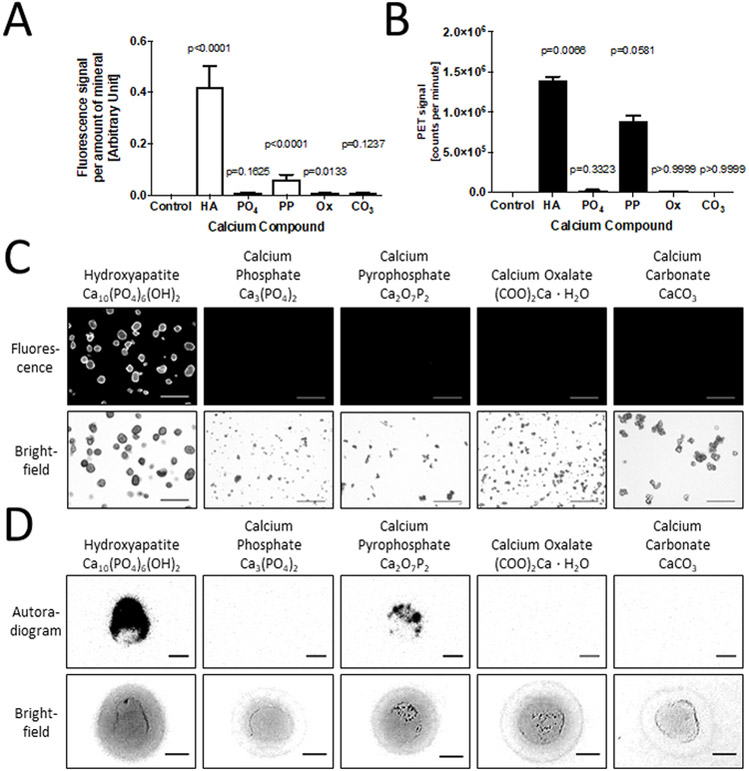
Methods: 18F-fluoride signal amplification derived from microcalcifications was validated against near-infrared fluorescence molecular imaging and histology using an in vitro 3-dimensional hydrogel collagen platform, ex vivo human specimens, and a mouse model of atherosclerosis.
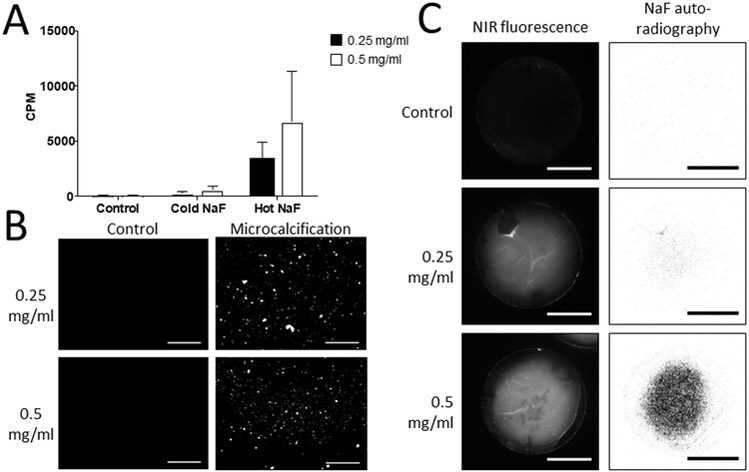
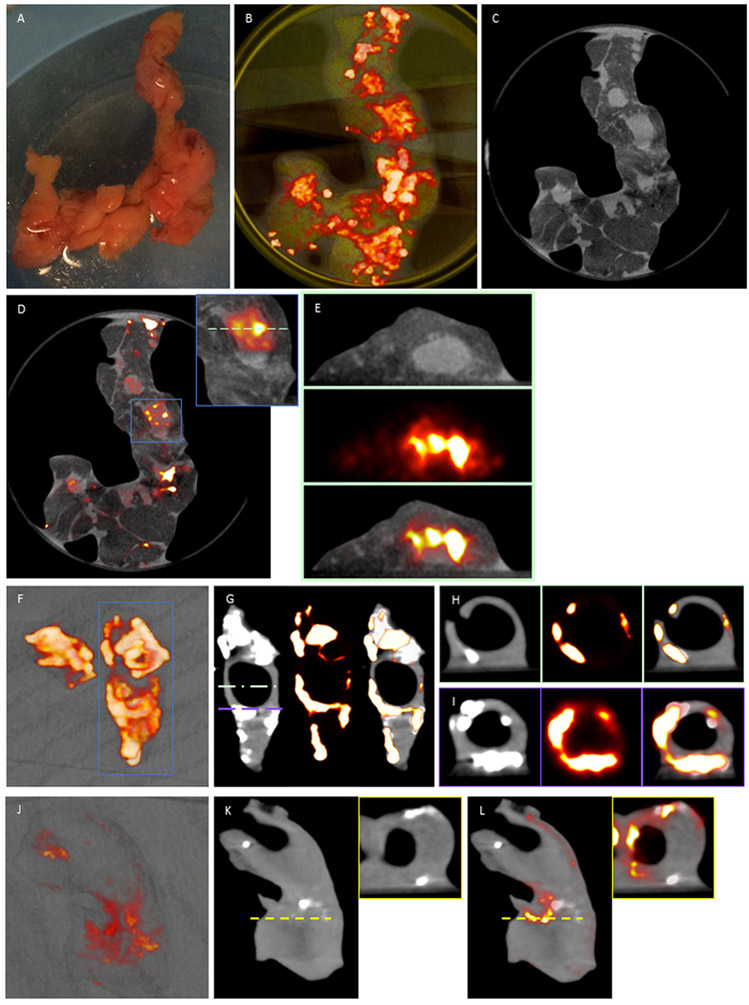
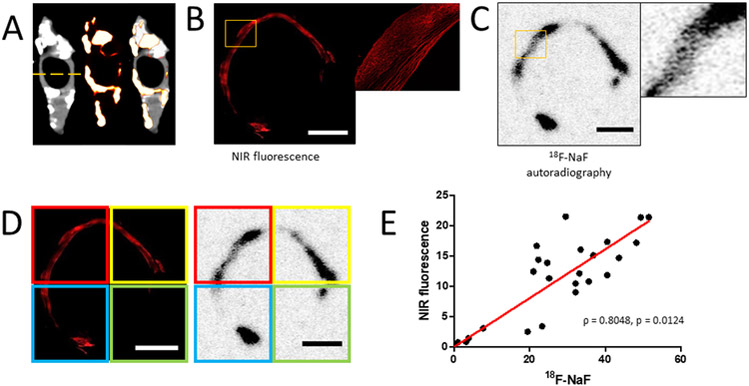
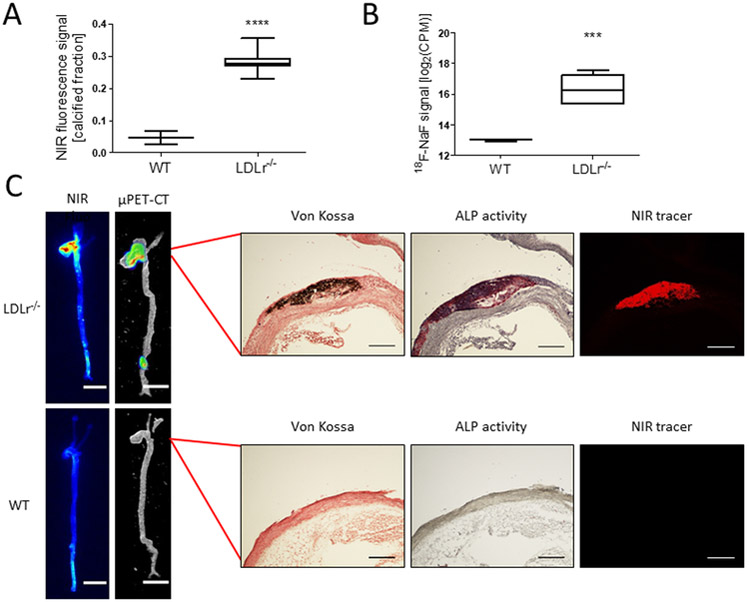
Results: Microcalcification size correlated inversely with collagen concentration. The 18F-fluoride ligand bound to microcalcifications formed by calcifying vascular smooth muscle cell derived extracellular vesicles in the in vitro 3-dimensional collagen system and exhibited an increasing signal with an increase in collagen concentration (0.25 mg/mL collagen -33.8×102±12.4×102 counts per minute; 0.5 mg/mL collagen -67.7×102±37.4×102 counts per minute; P=0.0014), suggesting amplification of the PET signal by smaller microcalcifications. We further incubated human atherosclerotic endarterectomy specimens with clinically relevant concentrations of 18F-fluoride. The 18F-fluoride ligand labeled microcalcifications in PET-positive, CT-negative regions of explanted human specimens as evidenced by 18F-fluoride PET/CT imaging, near-infrared fluorescence, and histological analysis. Additionally, the 18F-fluoride ligand identified micro and macrocalcifications in atherosclerotic aortas obtained from low-density lipoprotein receptor-deficient mice.
Conclusions: Our results suggest that 18F-fluoride PET signal in PET-positive, CT-negative regions of human atherosclerotic plaques is the result of developing microcalcifications, and high surface area in regions of small microcalcifications may amplify PET signal.
Keywords: atherosclerosis; fluoride; microcalcification; molecular imaging; positron emission tomography.
Figures
Comment in
-
18F-Sodium Fluoride Positron Emission Tomography and Plaque Calcification.Circ Cardiovasc Imaging. 2019 Jan;12(1):e008712. doi: 10.1161/CIRCIMAGING.118.008712. Circ Cardiovasc Imaging. 2019. PMID: 30642218 Free PMC article. No abstract available.
References
-
- Greenland P, LaBree L, Azen SP, Doherty TM and Detrano RC. Coronary artery calcium score combined with Framingham score for risk prediction in asymptomatic individuals. Jama. 2004;291:210–5. - PubMed
-
- Detrano R, Guerci AD, Carr JJ, Bild DE, Burke G, Folsom AR, Liu K, Shea S, Szklo M, Bluemke DA, O’Leary DH, Tracy R, Watson K, Wong ND and Kronmal RA. Coronary calcium as a predictor of coronary events in four racial or ethnic groups. The New England journal of medicine. 2008;358:1336–45. - PubMed
-
- Hecht HS, Cronin P, Blaha MJ, Budoff MJ, Kazerooni EA, Narula J, Yankelevitz D and Abbara S. 2016 SCCT/STR guidelines for coronary artery calcium scoring of noncontrast noncardiac chest CT scans: A report of the Society of Cardiovascular Computed Tomography and Society of Thoracic Radiology. Journal of cardiovascular computed tomography. 2017;11:74–84. - PubMed
-
- O’Brien KD, Kuusisto J, Reichenbach DD, Ferguson M, Giachelli C, Alpers CE and Otto CM. Osteopontin is expressed in human aortic valvular lesions. Circulation. 1995;92:2163–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
