

Serum uric acid and cardiovascular mortality in chronic kidney disease: a meta-analysis
- PMID: 30642279
- PMCID: PMC6330757
- DOI: 10.1186/s12882-018-1143-7
Serum uric acid and cardiovascular mortality in chronic kidney disease: a meta-analysis
Abstract
Background: Conflicting results have been reported from studies evaluating serum uric acid (SUA) levels as an independent risk factor for cardiovascular mortality in patients with chronic kidney disease (CKD).
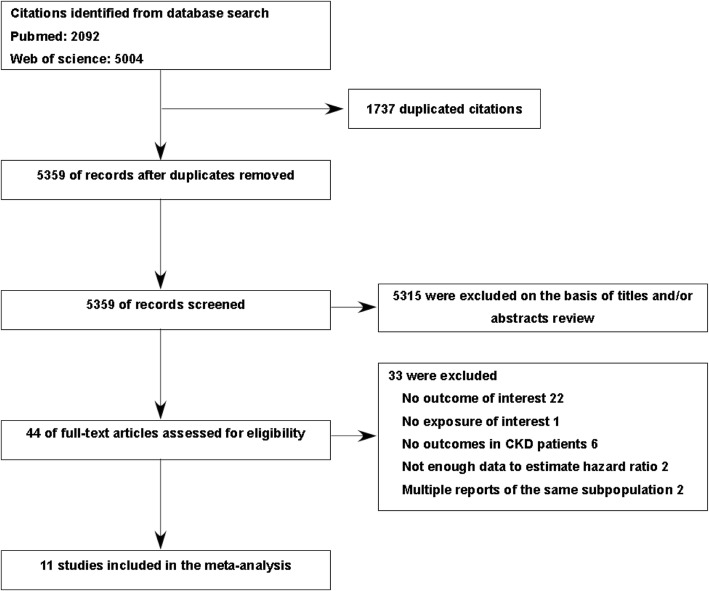
Methods: We systematically searched MEDLINE, Web of Science, and bibliographies of retrieved articles to identify studies reporting on the association between SUA levels and cardiovascular mortality in patients with CKD. Random-effects models were used to calculate the pooled hazard ratios (HR) and corresponding 95% confidence intervals (CI).
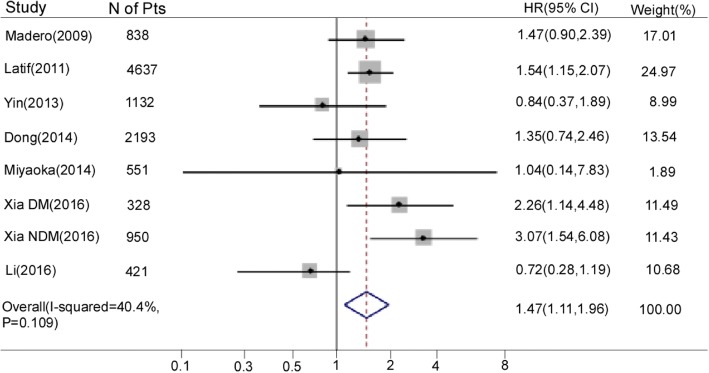
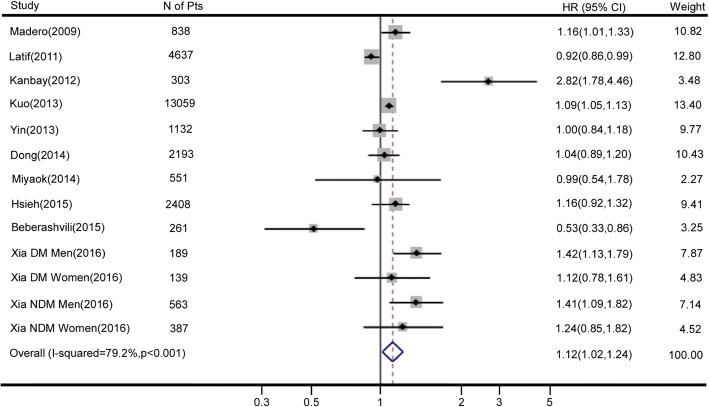
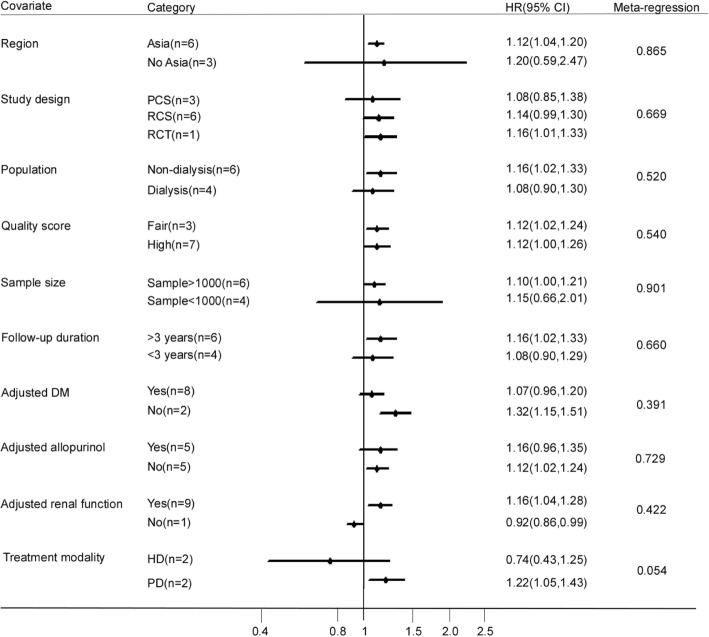
Results: We included 11 studies with an overall sample of 27,081 patients with CKD in this meta-analysis. By meta-analysis, restricted to 7 studies (n = 11,050), patients with the highest SUA were associated with an increased risk of cardiovascular mortality (HR 1.47, 95% CI 1.11-1.96) compared with patients with the lowest SUA. There was no indication of publication bias or significant heterogeneity (I2 = 40.4%; P = 0.109). Meta-analysis of 10 studies (n = 26,660) indicated that every 1 mg/dl increase in SUA levels increased a 12% risk in cardiovascular mortality (HR 1.12, 95% CI 1.02-1.24), with significant heterogeneity (I2 = 79.2%, P < 0.001).
Conclusions: Higher SUA levels are associated with significantly increased risk of cardiovascular mortality in patients with CKD. More designed studies, especially randomized controlled trials, should be conducted to determine whether high SUA levels is a potentially modifiable risk factor for cardiovascular mortality in patients with CKD.
Keywords: Cardiovascular mortality; Chronic kidney disease; Meta-analysis; Serum uric acid.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Association between mortality and serum uric acid levels in non-diabetes-related chronic kidney disease: An analysis of the National Health and Nutrition Examination Survey, USA, 1999-2010.Sci Rep. 2020 Oct 16;10(1):17585. doi: 10.1038/s41598-020-74747-w. Sci Rep. 2020. PMID: 33067501 Free PMC article.
-
Serum Uric Acid and Mortality in Patients with Chronic Kidney Disease: A Systematic Review and Meta-Analysis.Blood Purif. 2021;50(6):758-766. doi: 10.1159/000513944. Epub 2021 Mar 19. Blood Purif. 2021. PMID: 33744888
-
Serum uric acid level and all-cause and cardiovascular mortality in peritoneal dialysis patients: A systematic review and dose-response meta-analysis of cohort studies.PLoS One. 2022 Feb 22;17(2):e0264340. doi: 10.1371/journal.pone.0264340. eCollection 2022. PLoS One. 2022. PMID: 35192651 Free PMC article.
-
Elevated serum uric acid and risk of cardiovascular or all-cause mortality in maintenance hemodialysis patients: A meta-analysis.Nutr Metab Cardiovasc Dis. 2021 Feb 8;31(2):372-381. doi: 10.1016/j.numecd.2020.11.017. Epub 2020 Nov 25. Nutr Metab Cardiovasc Dis. 2021. PMID: 33485730
-
Baseline serum uric acid level as a predictor of cardiovascular disease related mortality and all-cause mortality: a meta-analysis of prospective studies.Atherosclerosis. 2013 Nov;231(1):61-8. doi: 10.1016/j.atherosclerosis.2013.08.023. Epub 2013 Aug 31. Atherosclerosis. 2013. PMID: 24125412 Review.
Cited by
-
Association between mortality and serum uric acid levels in non-diabetes-related chronic kidney disease: An analysis of the National Health and Nutrition Examination Survey, USA, 1999-2010.Sci Rep. 2020 Oct 16;10(1):17585. doi: 10.1038/s41598-020-74747-w. Sci Rep. 2020. PMID: 33067501 Free PMC article.
-
Hyperuricemia Is Associated with Left Ventricular Dysfunction and Inappropriate Left Ventricular Mass in Chronic Kidney Disease.Diagnostics (Basel). 2020 Jul 24;10(8):514. doi: 10.3390/diagnostics10080514. Diagnostics (Basel). 2020. PMID: 32722021 Free PMC article.
-
The Singapore Experience With Uncontrolled Gout: Unmet Needs in the Management of Patients.Cureus. 2023 Mar 25;15(3):e36682. doi: 10.7759/cureus.36682. eCollection 2023 Mar. Cureus. 2023. PMID: 36987445 Free PMC article. Review.
-
Management of Hyperuricemia in Patients with Chronic Kidney Disease: a Focus on Renal Protection.Curr Hypertens Rep. 2020 Oct 31;22(12):102. doi: 10.1007/s11906-020-01116-3. Curr Hypertens Rep. 2020. PMID: 33128170 Free PMC article. Review.
-
Interaction between anemia and hyperuricemia in the risk of all-cause mortality in patients with chronic kidney disease.Front Endocrinol (Lausanne). 2024 Mar 22;15:1286206. doi: 10.3389/fendo.2024.1286206. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 38586465 Free PMC article.
References
-
- Matsushita K, van der Velde M, Astor BC, et al. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet (London, England) 2010;375(9731):2073–2081. doi: 10.1016/S0140-6736(10)60674-5. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
