

Changes in the cohort composition of turner syndrome and severe non-diagnosis of Klinefelter, 47,XXX and 47,XYY syndrome: a nationwide cohort study
- PMID: 30642344
- PMCID: PMC6332849
- DOI: 10.1186/s13023-018-0976-2
Changes in the cohort composition of turner syndrome and severe non-diagnosis of Klinefelter, 47,XXX and 47,XYY syndrome: a nationwide cohort study
Abstract
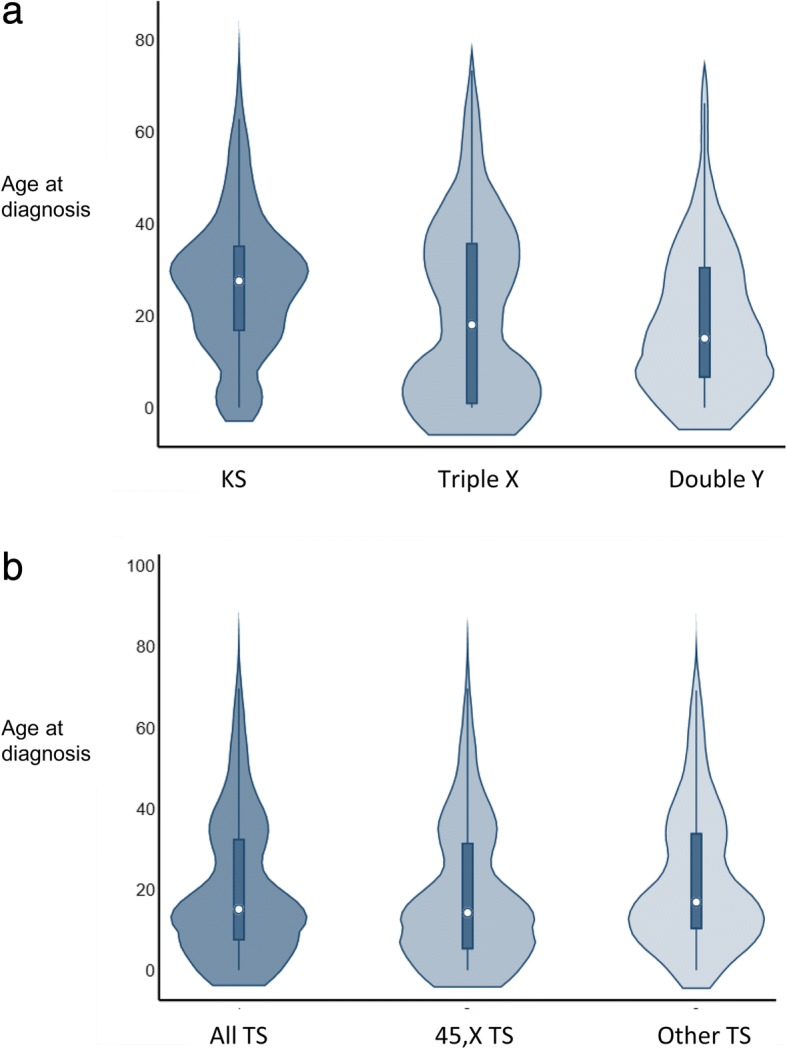
Background: Knowledge on the prevalence of sex chromosome abnormalities (SCAs) is limited, and delayed diagnosis or non-diagnosis of SCAs are a continuous concern. We aimed to investigate change over time in incidence, prevalence and age at diagnosis among Turner syndrome (TS), Klinefelter syndrome (KS), Triple X syndrome (Triple X) and Double Y syndrome (Double Y).
Methods: This study is a nationwide cohort study in a public health care system. The Danish Cytogenetic Central Registry (DCCR) holds information on all karyotypes performed in Denmark since 1961. We identified all individuals in the DCCR with a relevant SCA during 1961-2014; TS: n = 1156; KS: n = 1235; Triple X: n = 197; and Double Y: n = 287. From Statistics Denmark, which holds an extensive collection of data on the Danish population, complete data concerning dates of death and migrations in and out of Denmark were retrieved for all individuals.
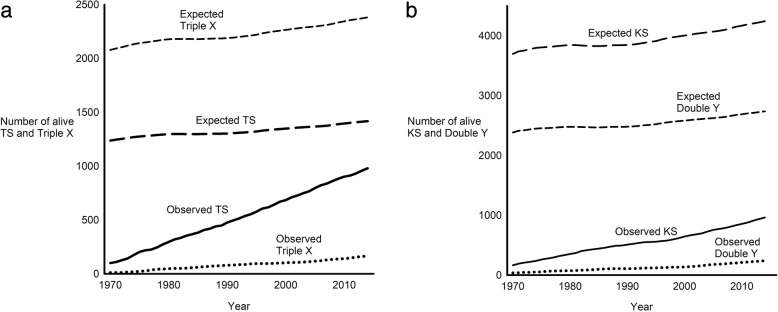
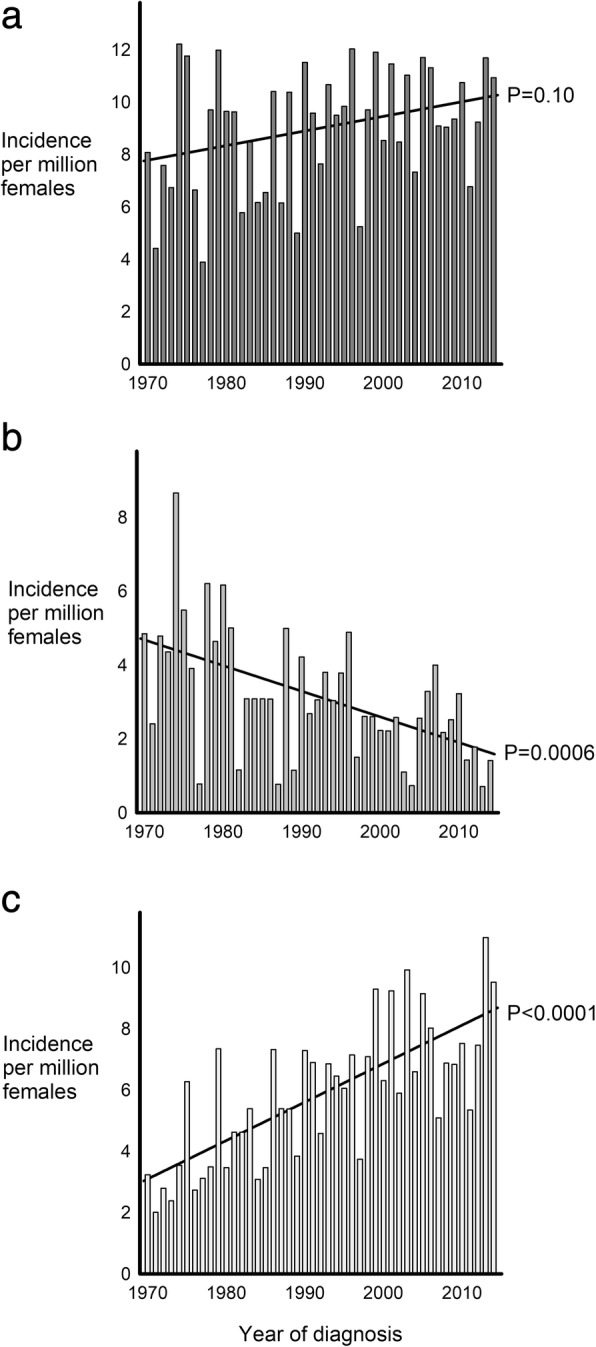
Results: The prevalence among newborns was as follows: TS: 59 per 100,000 females; KS: 57 per 100,000 males; Triple X: 11 per 100,000 females; and Double Y: 18 per 100,000 males. Compared with the expected number among newborns, all TS, 38% of KS, 13% of Triple X, and 18% of Double Y did eventually receive a diagnosis. The incidence of TS with other karyotypes than 45,X (P < 0.0001), KS (P = 0.02), and Double Y (P = 0.03) increased during the study period whereas the incidence of 45,X TS decreased (P = 0.0006). The incidence of Triple X was stable (P = 0.22).
Conclusions: The prevalence of TS is higher than previously identified, and the karyotypic composition of the TS population is changing. Non-diagnosis is extensive among KS, Triple X and Double Y, whereas all TS seem to become diagnosed. The diagnostic activity has increased among TS with other karyotypes than 45,X as well as among KS and Double Y.
Keywords: Age at diagnosis; Double Y syndrome; Incidence; Klinefelter syndrome; Prevalence; Triple X syndrome; Turner syndrome.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Danish Data Protection Agency (journal number: 2013-41-2017). According to Danish law no approval was obtained by the National Committee on Health Research Ethics since the study solely includes registry data.
Consent for publication
The manuscript contains no individual person’s data in any form.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Linden MG, Bender BG, Robinson A. Sex chromosome tetrasomy and pentasomy. Pediatrics. 1995;96:672–682. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
