

Positron emission tomography of tau in Iraq and Afghanistan Veterans with blast neurotrauma
- PMID: 30642757
- PMCID: PMC6412062
- DOI: 10.1016/j.nicl.2019.101651
Positron emission tomography of tau in Iraq and Afghanistan Veterans with blast neurotrauma
Abstract
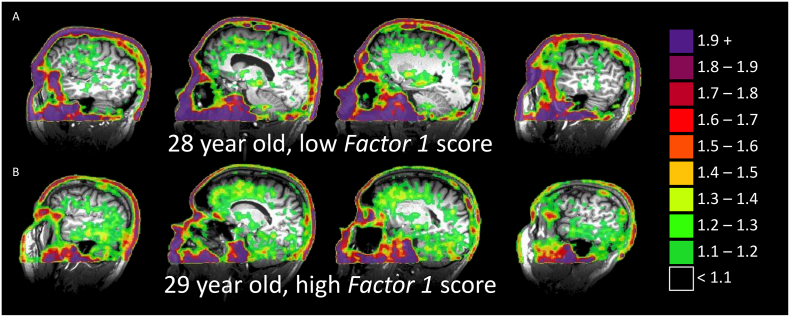
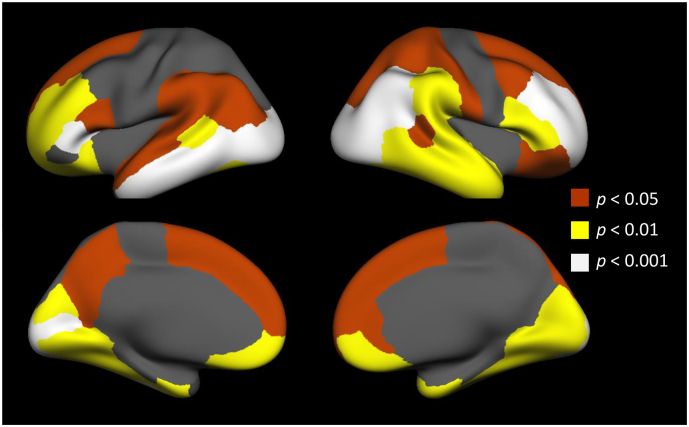
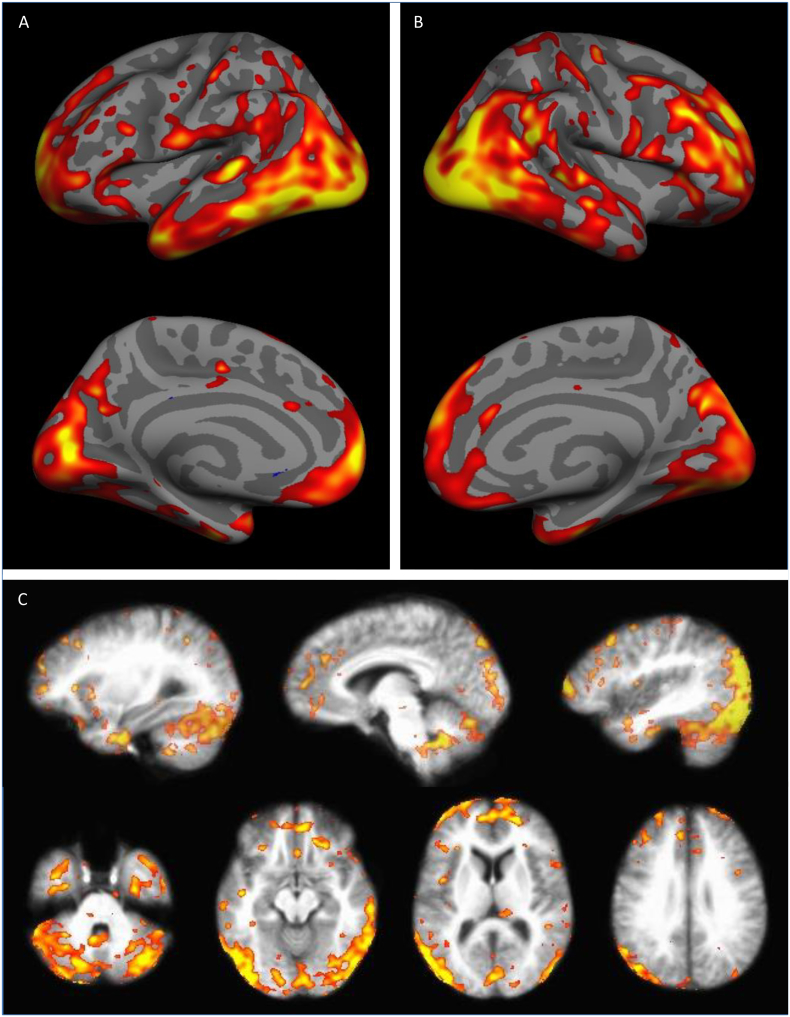
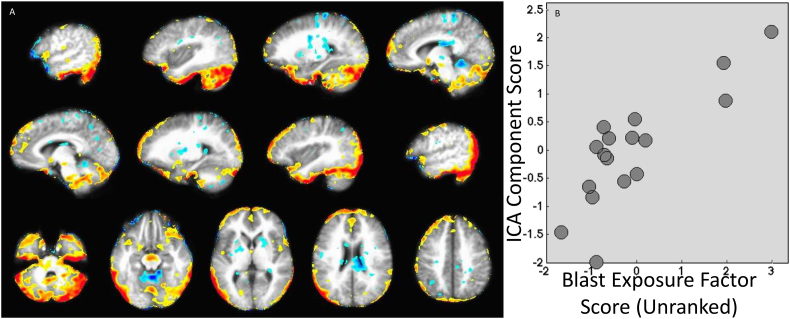
Military personnel are often exposed to multiple instances of various types of head trauma. As a result, there has been increasing concern recently over identifying when head trauma has resulted in a brain injury and what, if any, long-term consequences those brain injuries may have. Efforts to develop equipment to protect soldiers from these long-term consequences will first require understanding the types of head trauma that are likely responsible. In this study, we sought to identify the types of head trauma most likely to lead to the deposition of tau, a protein identified as a likely indicator of long-term negative consequences of brain injury. To define the types of head trauma in a military population, we applied a factor analysis to interviews from a larger cohort of 428 Veterans enrolled in the Translational Research Center for Traumatic Brain Injury and Stress Disorders. Three factors were identified: Blast Exposure, Symptom Duration, and Blunt Concussion. Sixteen male Veterans from this study and one additional male civilian (aged 25-69, mean 35.2 years) underwent simultaneous positron emission tomography/magnetic resonance imaging using a tracer that binds to tau protein, the ligand T807/AV-1451 (Flortaucipir). Standard uptake value ratios to the isthmus of the cingulate were calculated from a 20-minute time frame 70 min post-injection. We found that tracer uptake throughout the brain was associated with Blast Exposure factor beta weights, but not with either Symptom Duration or Blunt Concussion. Associations with uptake were located primarily in the cerebellar, occipital, inferior temporal and frontal regions. The data suggest that in this small, relatively young cohort of Veterans, elevated T807/AV-1451 uptake is associated with exposure to blast neurotrauma. These findings are unanticipated, as they do not match histopathological descriptions of tau pathology associated with head trauma. Continued work will be necessary to understand the nature of the regional T807/AV-1451 uptake and any associations with clinical symptoms.
Keywords: Blast; Positron emission tomography; Tau; Traumatic brain injury; Veteran.
Published by Elsevier Inc.
Figures
References
-
- Abbas K., Shenk T., Poole V., Breedlove E., Breedlove K., Leverenz L., Nauman E., Talavage T., Robinson M. Alteration of default mode network in high school football athletes due to repetitive sub-concussive mTBI. Brain Connect. 2014;5:91–1014. - PubMed
-
- Bailes Julian E., Petraglia Anthony L., Omalu Bennet I., Nauman Eric, Talavage Thomas. Role of subconcussion in repetitive mild traumatic brain injury. J. Neurosurg. 2013;119:1235–1245. - PubMed
-
- Baugh C.M., Stamm J.M., Riley D.O., Gavett B.E., Shenton M.E., Lin A., Nowinski C.J., Cantu R.C., McKee A.C., Stern R.A. Chronic traumatic encephalopathy: neurodegeneration following repetitive concussive and subconcussive brain trauma. Brain Imaging Behav. 2012;6:244–254. - PubMed
-
- Bazarian J., Donnelly K., Peterson D., Warner G., Zhu T., Zhong J. The relation between posttraumatic stress disorder and mild traumatic brain injury acquired during Operations Enduring Freedom and Iraqi Freedom. J. Head Trauma Rehabil. 2012;28:1–12. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
