

Optimizing the AKI definition during first postnatal week using Assessment of Worldwide Acute Kidney Injury Epidemiology in Neonates (AWAKEN) cohort
- PMID: 30643188
- PMCID: PMC6377843
- DOI: 10.1038/s41390-018-0249-8
Optimizing the AKI definition during first postnatal week using Assessment of Worldwide Acute Kidney Injury Epidemiology in Neonates (AWAKEN) cohort
Abstract
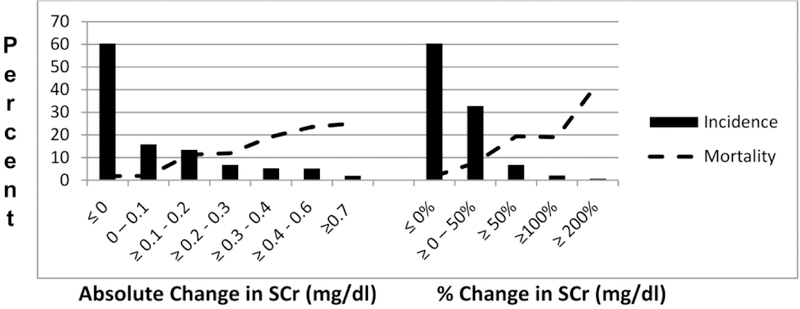
Background: Neonates with serum creatinine (SCr) rise ≥0.3 mg/dL and/or ≥50% SCr rise are more likely to die, even when controlling for confounders. These thresholds have not been tested in newborns. We hypothesized that different gestational age (GA) groups require different SCr thresholds.
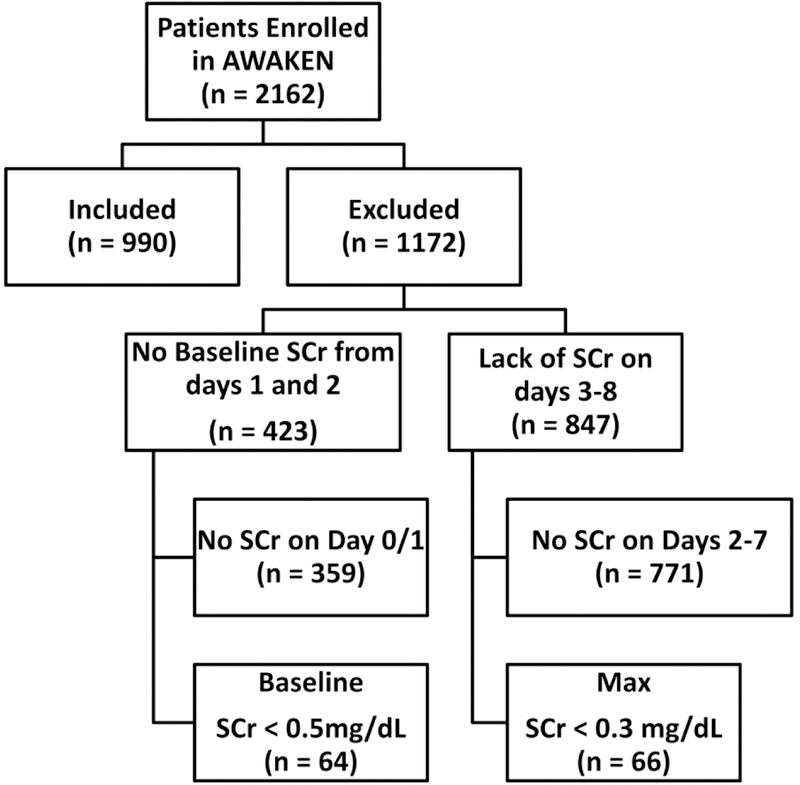
Methods: Neonates in Assessment of Worldwide Acute Kidney Epidemiology in Neonates (AWAKEN) with ≥1 SCr on postnatal days 1-2 and ≥1 SCr on postnatal days 3-8 were assessed. We compared the mortality predictability of SCr absolute (≥0.3 mg/dL) vs percent (≥50%) rise. Next, we determine usefulness of combining absolute with percent rise. Finally, we determined the optimal absolute, percent, and maximum SCr thresholds that provide the highest mortality area under curve (AUC) and specificity for different GA groups.
Results: The ≥0.3 mg/dL rise outperformed ≥50% SCr rise. Addition of percent rise did not improve mortality predictability. The optimal SCr thresholds to predict AUC and specificity were ≥0.3 and ≥0.6 mg/dL for ≤29 weeks GA, and ≥0.1 and ≥0.3 mg/dL for >29 week GA. The maximum SCr value provides great specificity.
Conclusion: Unique SCr rise cutoffs for different GA improves outcome prediction. Percent SCr rise does not add value to the neonatal AKI definition.
Conflict of interest statement
Conflict of interest disclosures
All authors declare no real or perceived conflicts of interest that could affect the study design, collection, analysis and interpretation of data, writing of the report, or the decision to submit for publication.
Figures
References
-
- Wong JH, Selewski DT, Yu S, et al. 2016. Severe Acute Kidney Injury Following Stage 1 Norwood Palliation: Effect on Outcomes and Risk of Severe Acute Kidney Injury at Subsequent Surgical Stages. Pediatr Crit Care Med 17:615–623. - PubMed
-
- Taylor ML, Carmona F, Thiagarajan RR, Westgate L, Ferguson MA, del Nido PJ, Rajagopal SK 2013. Mild postoperative acute kidney injury and outcomes after surgery for congenital heart disease. J Thorac Cardiovasc Surg 146:146–152. - PubMed
-
- dos Santos El Halal MG, Carvalho PR 2013. Acute kidney injury according to pediatric RIFLE criteria is associated with negative outcomes after heart surgery in children. Pediatr Nephrol 28:1307–1314. - PubMed
-
- Aydin SI, Seiden HS, Blaufox AD, Parnell VA, Choudhury T, Punnoose A, Schneider J 2012. Acute kidney injury after surgery for congenital heart disease. Ann Thorac Surg 94:1589–1595. - PubMed
-
- Mathur NB, Agarwal HS, Maria A 2006. Acute renal failure in neonatal sepsis. Indian J Pediatr 73:499–502. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
