

BOADICEA: a comprehensive breast cancer risk prediction model incorporating genetic and nongenetic risk factors
- PMID: 30643217
- PMCID: PMC6687499
- DOI: 10.1038/s41436-018-0406-9
BOADICEA: a comprehensive breast cancer risk prediction model incorporating genetic and nongenetic risk factors
Erratum in
-
Correction: BOADICEA: a comprehensive breast cancer risk prediction model incorporating genetic and nongenetic risk factors.Genet Med. 2019 Jun;21(6):1462. doi: 10.1038/s41436-019-0459-4. Genet Med. 2019. PMID: 30787466 Free PMC article.
Abstract
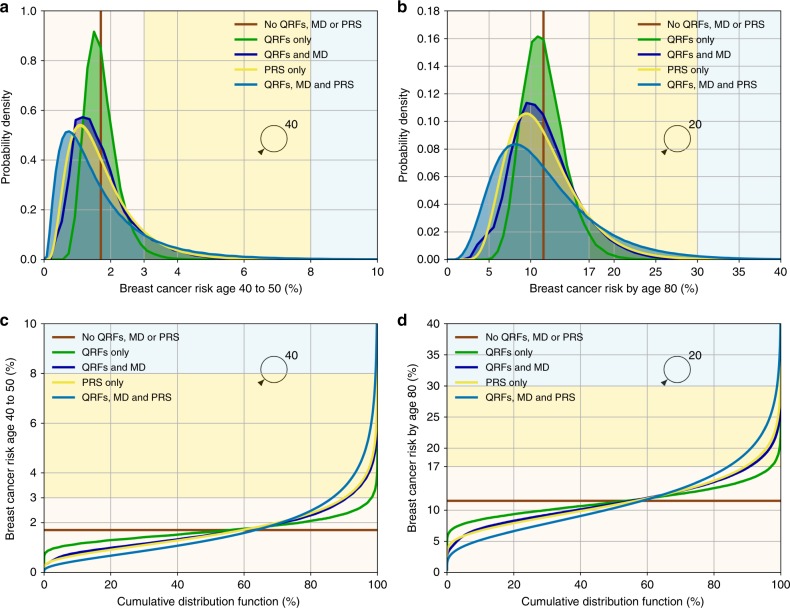
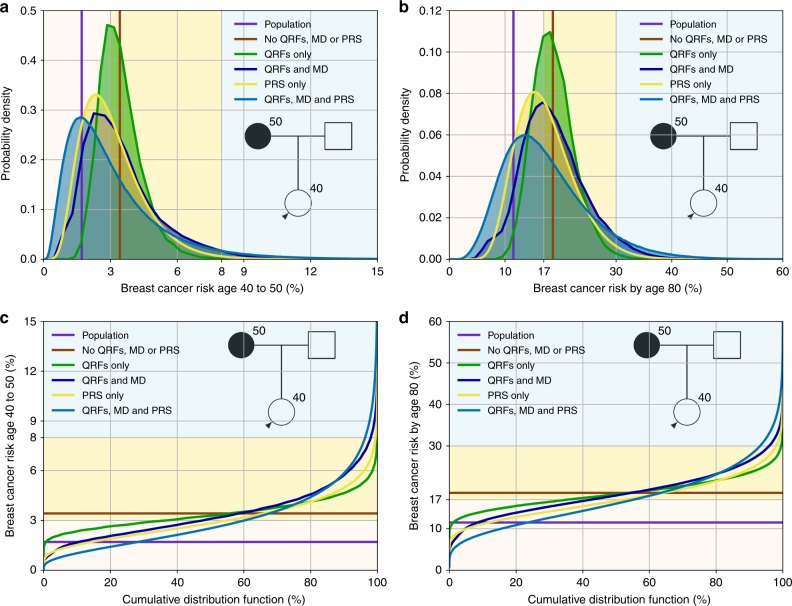
Purpose: Breast cancer (BC) risk prediction allows systematic identification of individuals at highest and lowest risk. We extend the Breast and Ovarian Analysis of Disease Incidence and Carrier Estimation Algorithm (BOADICEA) risk model to incorporate the effects of polygenic risk scores (PRS) and other risk factors (RFs).
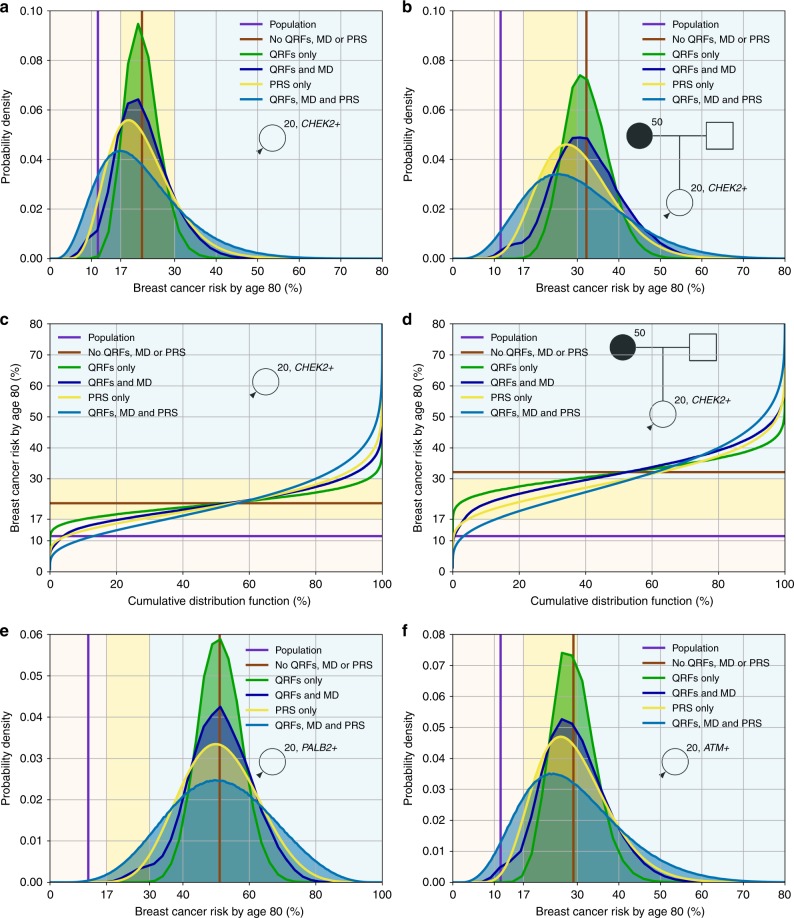
Methods: BOADICEA incorporates the effects of truncating variants in BRCA1, BRCA2, PALB2, CHEK2, and ATM; a PRS based on 313 single-nucleotide polymorphisms (SNPs) explaining 20% of BC polygenic variance; a residual polygenic component accounting for other genetic/familial effects; known lifestyle/hormonal/reproductive RFs; and mammographic density, while allowing for missing information.
Results: Among all factors considered, the predicted UK BC risk distribution is widest for the PRS, followed by mammographic density. The highest BC risk stratification is achieved when all genetic and lifestyle/hormonal/reproductive/anthropomorphic factors are considered jointly. With all factors, the predicted lifetime risks for women in the UK population vary from 2.8% for the 1st percentile to 30.6% for the 99th percentile, with 14.7% of women predicted to have a lifetime risk of ≥17-<30% (moderate risk according to National Institute for Health and Care Excellence [NICE] guidelines) and 1.1% a lifetime risk of ≥30% (high risk).
Conclusion: This comprehensive model should enable high levels of BC risk stratification in the general population and women with family history, and facilitate individualized, informed decision-making on prevention therapies and screening.
Keywords: BOADICEA; PRS; breast cancer; rare variants; risk prediction.
Figures
References
-
- National Institute for Health and Care Excellence. Familial breast cancer: classification and care of people at risk of familial breast cancer and management of breast cancer and related risks in people with a family history of breast cancer (CG164). 2013. http://www.nice.org.uk/CG164. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- 203477/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- 203477/B/16/Z/WT_/Wellcome Trust/United Kingdom
- C1287/A16563/CRUK_/Cancer Research UK/United Kingdom
- 20861/CRUK_/Cancer Research UK/United Kingdom
- MR/P012930/1/MRC_/Medical Research Council/United Kingdom
- A11174/CRUK_/Cancer Research UK/United Kingdom
- 16563/CRUK_/Cancer Research UK/United Kingdom
- 10119/CRUK_/Cancer Research UK/United Kingdom
- NIHR-CS-012-03/DH_/Department of Health/United Kingdom
- A20861/CRUK_/Cancer Research UK/United Kingdom
- C12292/A20861 /CRUK_/Cancer Research UK/United Kingdom
- 16561/CRUK_/Cancer Research UK/United Kingdom
- 10124/CRUK_/Cancer Research UK/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
