

Is COPD associated with alterations in hearing? A systematic review and meta-analysis
- PMID: 30643401
- PMCID: PMC6312399
- DOI: 10.2147/COPD.S182730
Is COPD associated with alterations in hearing? A systematic review and meta-analysis
Abstract
Background and aims: COPD is an irreversible or persistent airflow obstruction, which affects up to 600 million people globally. The primary purpose of this systematic review was to explore the COPD-based alteration in the auditory system function by conducting a quantitative analysis of presently published data.
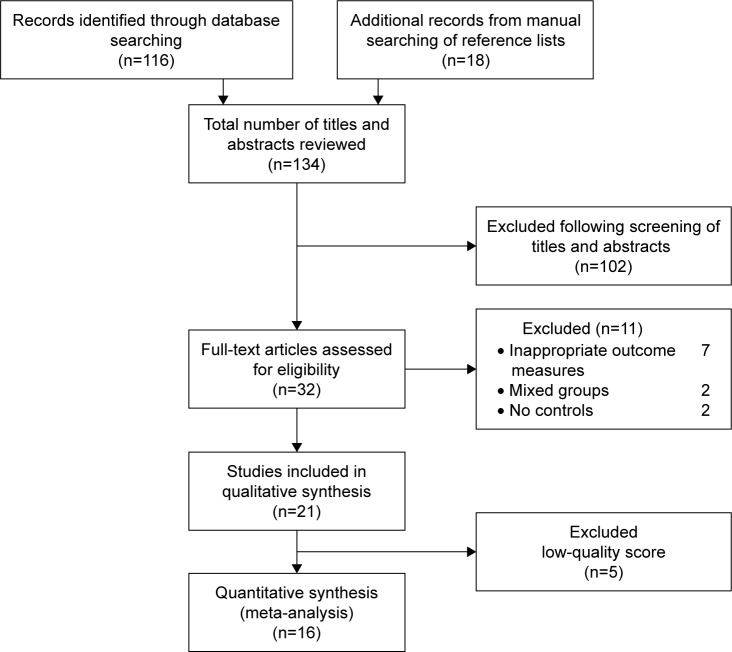
Materials and methods: We systematically searched seven diverse electronic databases and manual searching of references to identify relevant studies. Data from the selected studies were rated by two investigators independently in a blinded fashion. Meta-analysis was done on pooled data using Cochrane's Review Manager 5.3.
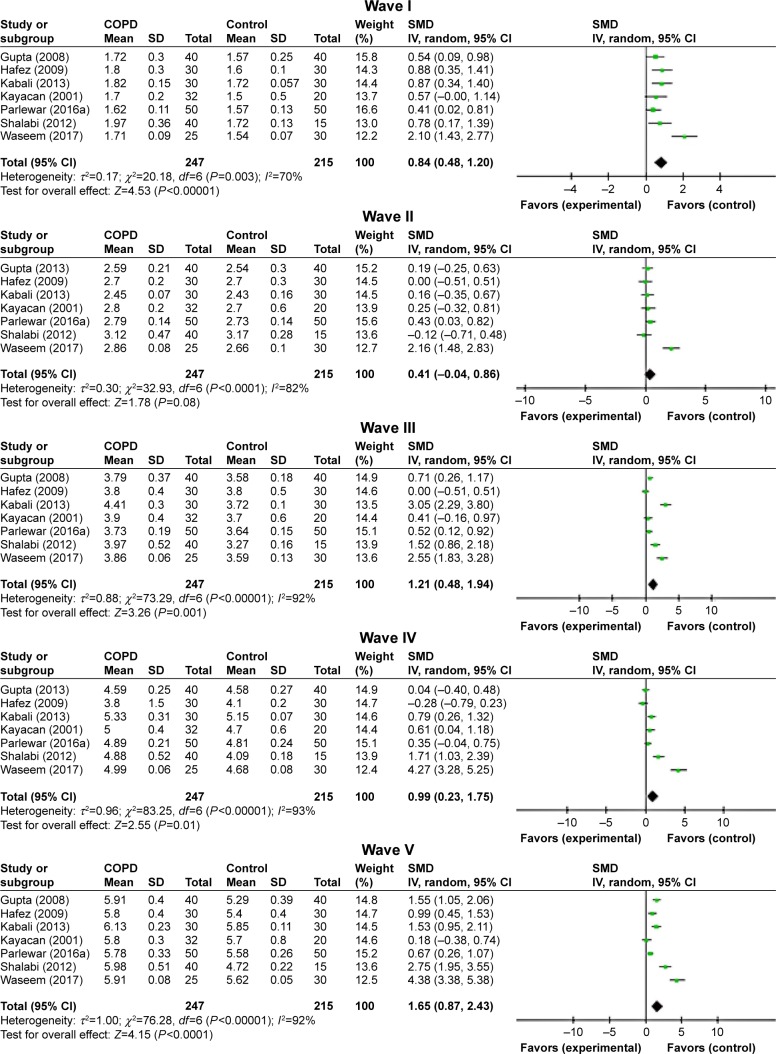
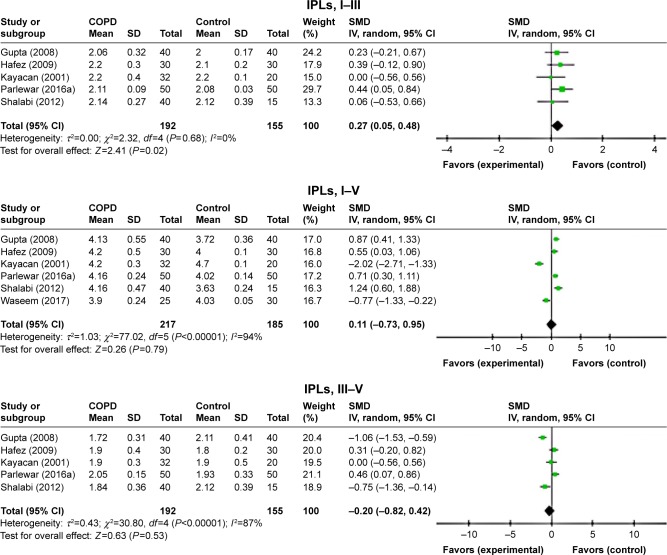
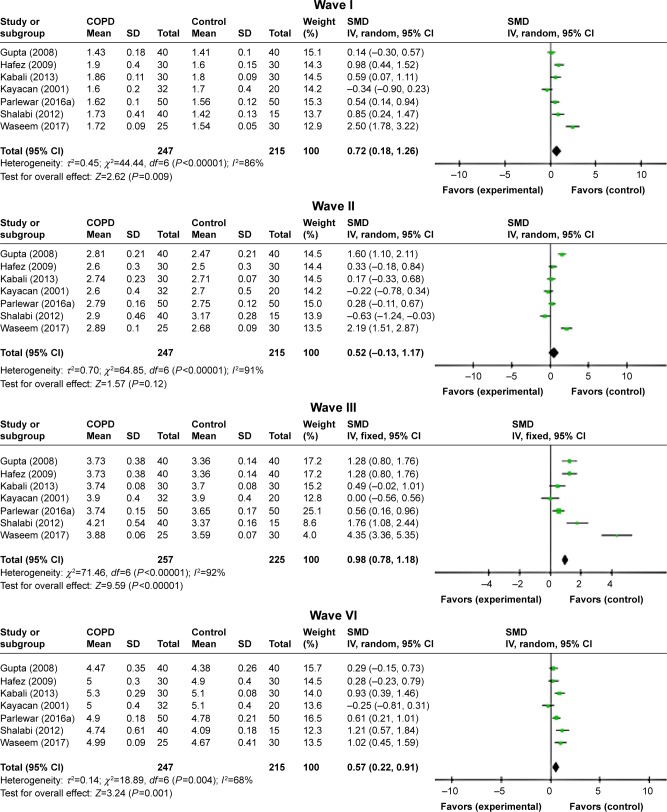
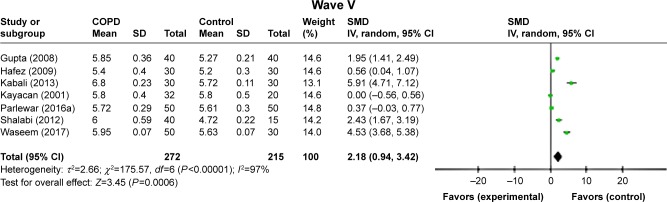
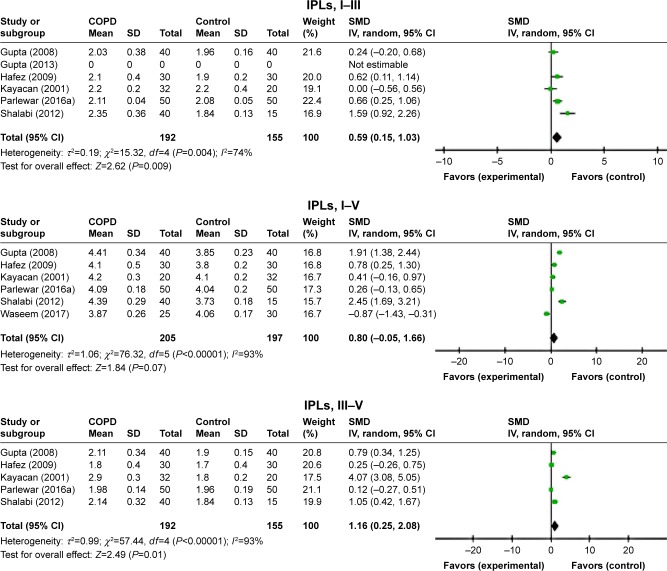
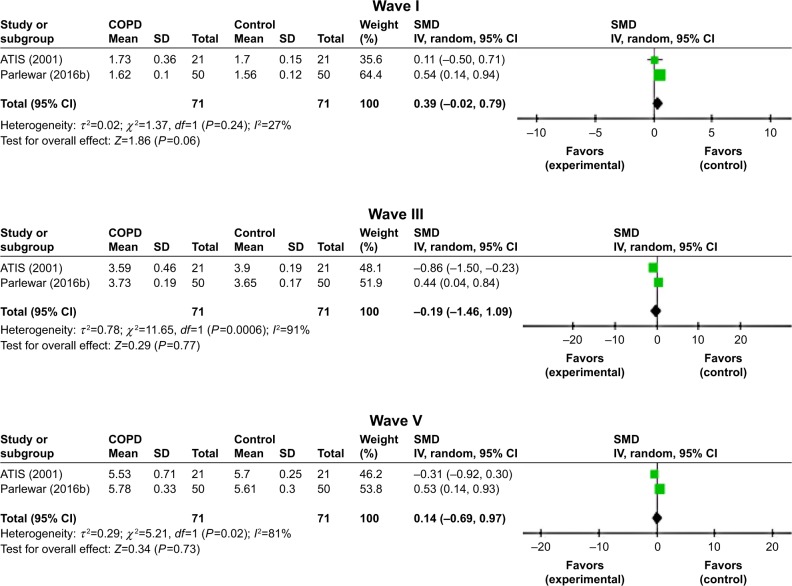
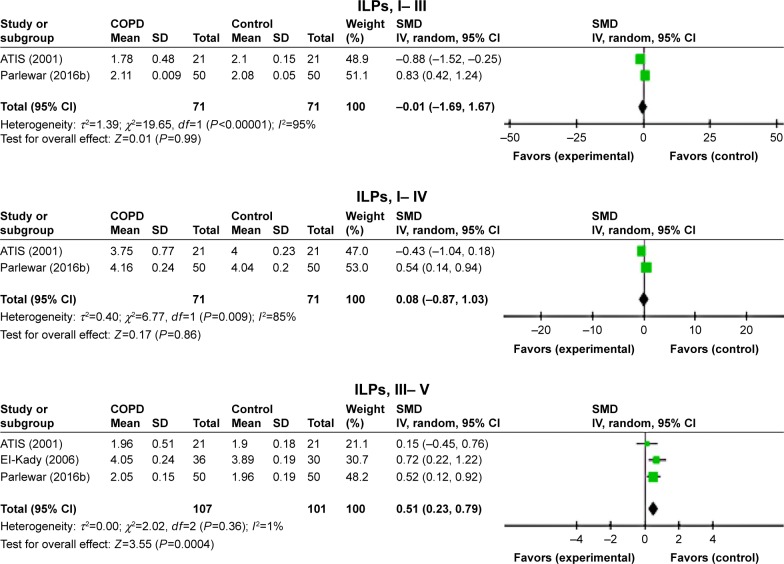
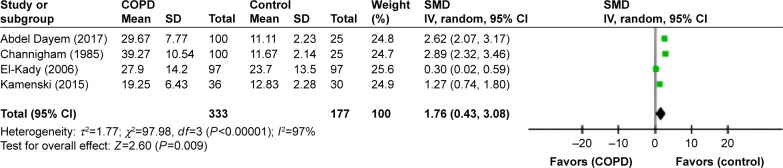
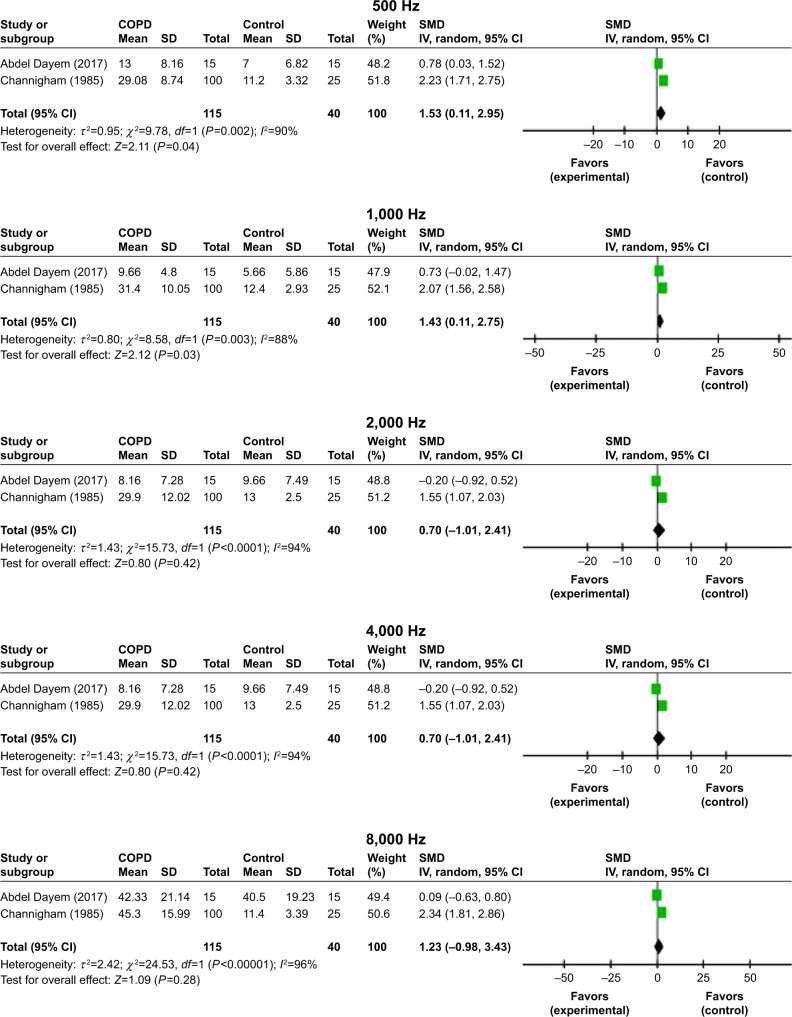
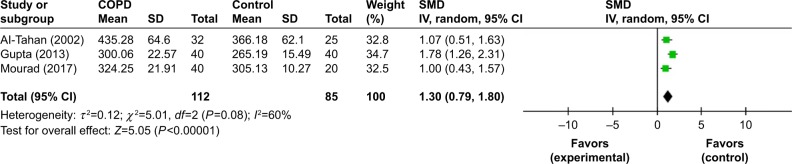
Results: Sixteen articles received suitable scores and were thus included for further processes. Hearing loss (HL) was defined as a change in pure tone audiometry (PTA) thresholds, auditory brainstem response (ABR), and auditory P300 parameters. ABR wave was significantly elongated in patients with COPD than in controls (standardized mean difference [SMD]=0.27, 95% CI: 0.05-0.48, P=0.02). PTA was significantly higher in patients with COPD when compared with controls (SMD=1.76, 95% CI: 0.43-3.08, P=0.0004). We found that patients with COPD had a significantly higher latency than controls (SMD=1.30, 95% CI: 0.79-1.80, P=0.0001).
Conclusion: COPD patients had considerably greater incidence of HL when compared with controls. Interestingly, although the mean PTA thresholds at every frequency for COPD patients were higher than those for controls, these values were still in the slight to mild HL ranges. Prolonged ABR wave latencies in the COPD patients suggest retro-cochlear involvement. Thus, COPD most frequently clusters with HL, but it is worth noting that alteration in hearing is not always recognized by medical experts as a frequent comorbidity associated with COPD.
Keywords: COPD; hearing loss; meta-analysis; systematic review.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
Comment in
-
Costen's syndrome and COPD.Int J Chron Obstruct Pulmon Dis. 2019 Feb 18;14:457-460. doi: 10.2147/COPD.S200787. eCollection 2019. Int J Chron Obstruct Pulmon Dis. 2019. PMID: 30863046 Free PMC article. No abstract available.
References
-
- Wilkinson TM, Donaldson GC, Hurst JR, Seemungal TA, Wedzicha JA. Early therapy improves outcomes of exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2004;169(12):1298–1303. - PubMed
-
- Schou L, Østergaard B, Rasmussen LS, Rydahl-Hansen S, Phanareth K. Cognitive dysfunction in patients with chronic obstructive pulmonary disease – a systematic review. Respir Med. 2012;106(8):1071–1081. - PubMed
-
- Ortapamuk H, Naldoken S. Brain perfusion abnormalities in chronic obstructive pulmonary disease: comparison with cognitive impairment. Ann Nucl Med. 2006;20(2):99–106. - PubMed
-
- El-Kady MA, Durrant JD, Tawfik S, Abdel-Ghany S, Moussa AM. Study of auditory function in patients with chronic obstructive pulmonary diseases. Hear Res. 2006;212(1–2):109–116. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
