

Post-Stroke Lingual Dystonia: Clinical Description and Neuroimaging Findings
- PMID: 30643669
- PMCID: PMC6329777
- DOI: 10.7916/D8RB8NJC
Post-Stroke Lingual Dystonia: Clinical Description and Neuroimaging Findings
Abstract
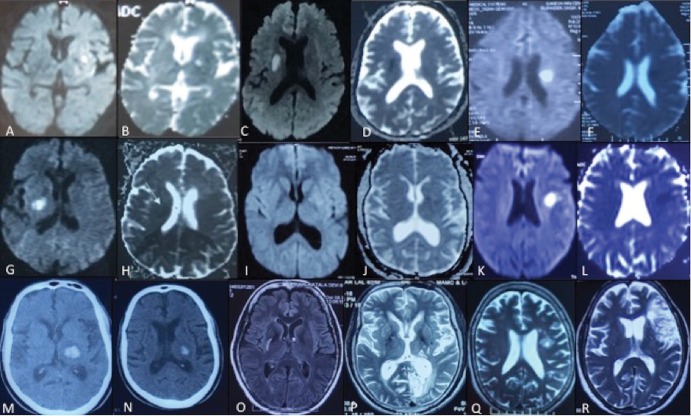
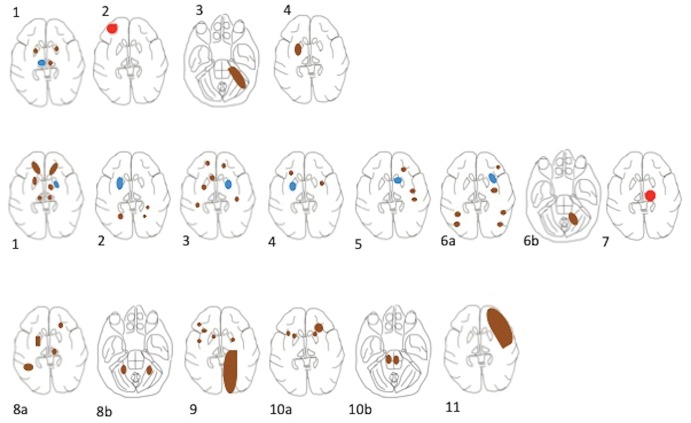
Background: Lingual dystonia is extremely rare following stroke. We describe clinical features and neuroimaging findings in a series of 11 patients (seven acute and four chronic) with post-stroke lingual dystonia and review the literature.
Methods: This was a case series using a preformed structured proforma and review of literature using a PubMed search.
Results: In our case series, all patients had dysarthria as a presenting symptom. Seven patients had acute presentation (six had an ischemic infarct and one had thalamic hemorrhage) and four had chronic presentation (all had infarct). All patients except one had small infarcts, with the majority of them in the basal ganglia and subcortical white matter regions. Additional chronic ischemic lesions were seen in all patients with acute presentation. The majority of the patients with acute (five out of seven; 71.42%) presentation had left-sided involvement on imaging. We could identify only one case of acute post-stroke lingual dystonia following the PubMed search. Three other cases of post-stroke lingual dystonia with chronic presentation have been described; however, these were associated with oromandibular or cranial dystonia.
Discussion: Our results, based on brain lesions, suggest that all lingual dystonia patients with acute infarcts had underlying chronic infarcts. Overall, more left-sided than right-sided strokes were observed with post-stroke lingual movement disorders including dystonia; however, the data were not significant (p = 1). All patients had dysarthria, with only one having mild tongue weakness and only four having facial weakness. This suggests that the lingual dystonia was responsible for the dysarthria rather than weakness in these patients.
Keywords: Dystonia; magnetic resonance images; stroke.
Conflict of interest statement
Funding: None. Conflicts of Interest: The authors report no conflict of interest. Ethics Statement: This study was performed in accordance with the ethical standards detailed in the Declaration of Helsinki. The authors’ institutional ethics committee has approved this study and all patients have provided written informed consent.
Figures
Similar articles
-
Lingual Dystonia Following Thalamic Infarction in a Patient on Methotrexate Therapy for Hidradenitis Suppurativa.Cureus. 2025 Apr 25;17(4):e82974. doi: 10.7759/cureus.82974. eCollection 2025 Apr. Cureus. 2025. PMID: 40416235 Free PMC article.
-
Dysarthria due to supratentorial and infratentorial ischemic stroke: a diffusion-weighted imaging study.Cerebrovasc Dis. 2007;23(5-6):331-8. doi: 10.1159/000099131. Epub 2007 Jan 30. Cerebrovasc Dis. 2007. PMID: 17268163
-
MRI-Based Neuroanatomical Predictors of Dysphagia, Dysarthria, and Aphasia in Patients with First Acute Ischemic Stroke .Cerebrovasc Dis Extra. 2017;7(1):21-34. doi: 10.1159/000457810. Epub 2017 Feb 16. Cerebrovasc Dis Extra. 2017. PMID: 28208139 Free PMC article.
-
Cervico-shoulder dystonia following lateral medullary infarction: a case report and review of the literature.J Med Case Rep. 2018 Feb 10;12(1):34. doi: 10.1186/s13256-018-1561-y. J Med Case Rep. 2018. PMID: 29426369 Free PMC article. Review.
-
Post-Thalamic Stroke Movement Disorders: A Systematic Review.Eur Neurol. 2018;79(5-6):303-314. doi: 10.1159/000490070. Epub 2018 Jun 5. Eur Neurol. 2018. PMID: 29870983
Cited by
-
Lingual Dystonia Following Thalamic Infarction in a Patient on Methotrexate Therapy for Hidradenitis Suppurativa.Cureus. 2025 Apr 25;17(4):e82974. doi: 10.7759/cureus.82974. eCollection 2025 Apr. Cureus. 2025. PMID: 40416235 Free PMC article.
-
A microstructural neural network biomarker for dystonia diagnosis identified by a DystoniaNet deep learning platform.Proc Natl Acad Sci U S A. 2020 Oct 20;117(42):26398-26405. doi: 10.1073/pnas.2009165117. Epub 2020 Oct 1. Proc Natl Acad Sci U S A. 2020. PMID: 33004625 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases