

Routinely staging gastric cancer with 18F-FDG PET-CT detects additional metastases and predicts early recurrence and death after surgery
- PMID: 30643947
- PMCID: PMC6443603
- DOI: 10.1007/s00330-018-5904-2
Routinely staging gastric cancer with 18F-FDG PET-CT detects additional metastases and predicts early recurrence and death after surgery
Abstract
Objectives: Fluorodeoxyglucose (FDG) positron emission tomography-computed tomography (PET-CT) is typically considered to have minimal yield in gastric cancer, and so is not consistently recommended by international guidelines. However, its yield is considerable in esophageal and junctional cancer, identifying unsuspected metastases and risk-stratifying patients using metabolic nodal stage (mN). We aimed to determine the contemporary utility of routine 18F-FDG PET-CT in gastric cancer.
Methods: We routinely stage patients with non-junctional gastric cancer with PET-CT, provided initial CT does not demonstrate unequivocal metastases. We performed a retrospective study of all such patients staged in our institution from January 2007 to July 2016. Our primary endpoint was detection of incurable disease. Our secondary endpoint was disease-free survival following gastrectomy. Decision theory, economic, and predictive models were generated.
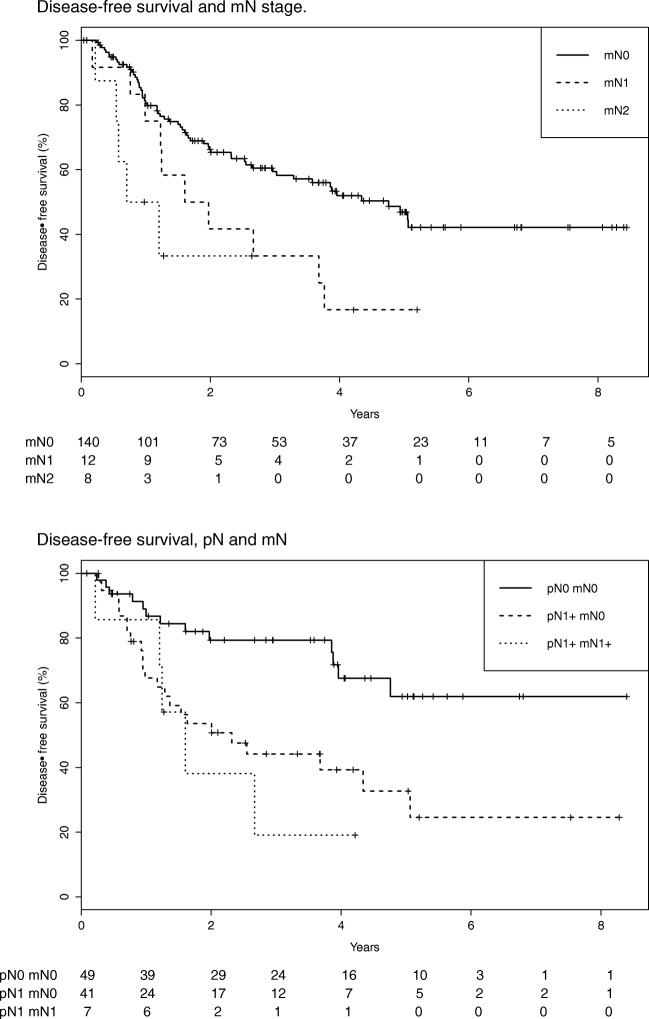
Results: The primary tumor was FDG-avid in 225/279 patients (80.6%). Seventy-two (25.8%) had FDG-avid nodes (resectable by D2 lymphadenectomy). This was not influenced by the Lauren classification. Unsuspected metastases were identified in 20 patients (7.2%). In 13 (4.7%), these would not have been otherwise identified. Decision theory and economic modeling supported routine PET-CT. Patients with FDG-avid nodes were more likely to have incurable disease (51.4% versus 15.5%; p < 0.001), and a worse prognosis if not: multivariate hazard ratio 2.19 (1.23-3.91; p = 0.008). Prognosis worsened with mN stage.
Conclusions: PET-CT appears useful when used routinely for non-junctional gastric cancer, and should be considered in international recommendations. Any extra costs appear small and offset by avoiding futile investigations and radical treatment. mN stage identifies patients at risk of early recurrence and death.
Key points: • PET-CT is typically not considered useful when staging gastric cancer. We describe a retrospective study of 279 patients routinely staged with PET-CT in the absence of metastases on CT. • The primary tumor was avid in 80% of patients. Twenty-five percent had resectable avid nodes. PET-CT identified previously unsuspected metastases in 7% of patients, which would likely not have been identified by conventional staging without PET-CT in 5%. These patients were much more likely to have avid nodes. • Beyond avoiding futile investigations and radical treatment in this 5%, we found patients with FDG-avid nodes (metabolic nodal stage, mN) to have a worse disease-free survival after gastrectomy.
Keywords: Cancer staging; Gastric cancer; Metastases; PET-CT; Prognosis.
Conflict of interest statement
Guarantor
The scientific guarantor of this publication is John Findlay.
Conflict of interest
The authors of this manuscript declare relationships with the following companies:
MRM has the following roles to disclose:
Advisory/consulting role (payment to the individual) Amgen, BMS, GSK, Merck, Millennium, Physiomics, and Roche. Research funding (payment to the institution) from Amgen, AZ, BMS, Clovis, Eisai, GSK, Immunocore, Johnson & Johnson, Merck, Millennium, Novartis, Pfizer, Roche, and Vertex. JMF has the following roles to disclose: Unremunerated advisory role to Physiomics
Statistics and biometry
One of the authors (JMF) has significant statistical expertise.
Informed consent
Written informed consent was waived by the Institutional Review Board.
Ethical approval
Institutional Review Board approval was obtained.
Methodology
• retrospective
• diagnostic or prognostic study
• performed at one institution
References
-
- Findlay JM, Bradley KM, Maile EJ et al (2015) Pragmatic staging of oesophageal cancer using decision theory involving selective endoscopic ultrasonography, PET and laparoscopy. Br J Surg 102:1488–1499. 10.1002/bjs.9905 - PubMed
-
- Findlay JM, Gillies RS, Franklin JM et al (2016) Restaging oesophageal cancer after neoadjuvant therapy with F-FDG PET-CT: identifying interval metastases and predicting incurable disease at surgery. Eur Radiol. 10.1007/s00330-016-4227-4 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
