

Association of Inferior Vena Cava Filter Placement for Venous Thromboembolic Disease and a Contraindication to Anticoagulation With 30-Day Mortality
- PMID: 30646021
- PMCID: PMC6324296
- DOI: 10.1001/jamanetworkopen.2018.0452
Association of Inferior Vena Cava Filter Placement for Venous Thromboembolic Disease and a Contraindication to Anticoagulation With 30-Day Mortality
Abstract
Importance: Despite the absence of data from randomized clinical trials, professional societies recommend inferior vena cava (IVC) filters for patients with venous thromboembolic disease (VTE) and a contraindication to anticoagulation therapy. Prior observational studies of IVC filters have suggested a mortality benefit associated with IVC filter insertion but have often failed to adjust for immortal time bias, which is the time before IVC filter insertion, during which death can only occur in the control group.
Objective: To determine the association of IVC filter placement with 30-day mortality after adjustment for immortal time bias.
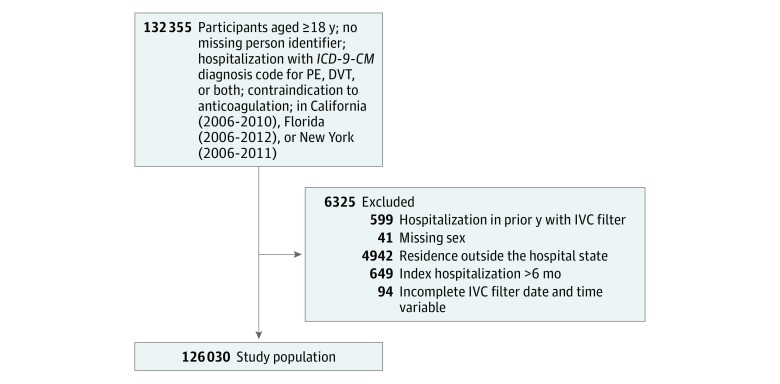
Design, setting, and participants: This comparative effectiveness, retrospective cohort study used a population-based sample of hospitalized patients with VTE and a contraindication to anticoagulation using the State Inpatient Database and the State Emergency Department Database, part of the Healthcare Cost and Utilization Project of the Agency for Healthcare Research and Quality, from hospitals in California (January 1, 2005, to December 31, 2011), Florida (January 1, 2005, to December 31, 2013), and New York (January 1, 2005, to December 31, 2012). Data analysis was conducted from September 15, 2015, to March 14, 2018.
Exposure: Inferior vena cava filter placement.
Main outcomes and measures: Multivariable Cox proportional hazard models were constructed with IVC filters as a time-dependent variable that adjusts for immortal time bias. The Cox model was further adjusted using the propensity score as an adjustment variable.
Results: Of 126 030 patients with VTE, 61 281 (48.6%) were male and the mean (SD) age was 66.9 (16.6) years. In this cohort, 45 771 (36.3%) were treated with an IVC filter, whereas 80 259 (63.7%) did not receive a filter. In the Cox model with IVC filter status analyzed as a time-dependent variable to account for immortal time bias, IVC filter placement was associated with a significantly increased hazard ratio of 30-day mortality (1.18; 95% CI, 1.13-1.22; P < .001). When the propensity score was included in the Cox model, IVC filter placement remained associated with an increased hazard ratio of 30-day mortality (1.18; 95% CI, 1.13-1.22; P < .001).
Conclusions and relevance: After adjustment for immortal time bias, IVC filter placement was associated with increased 30-day mortality in patients with VTE and a contraindication to anticoagulation. Randomized clinical trials are needed to determine the efficacy of IVC filter placement in patients with VTE and a contraindication to anticoagulation.
Conflict of interest statement
Figures
Comment in
-
Inferior Vena Cava Filters and Mortality: Is It the Underlying Process, the Patient, or the Device?JAMA Netw Open. 2018 Jul 6;1(3):e180453. doi: 10.1001/jamanetworkopen.2018.0453. JAMA Netw Open. 2018. PMID: 30646019 No abstract available.
-
Pulmonary Embolism: Controversies in Therapeutic Management.Am J Respir Crit Care Med. 2020 Jan 15;201(2):240-242. doi: 10.1164/rccm.201812-2357RR. Am J Respir Crit Care Med. 2020. PMID: 31794251 No abstract available.
References
-
- Heit JA. The epidemiology of venous thromboembolism in the community: implications for prevention and management. J Thromb Thrombolysis. 2006;21(1):-. - PubMed
-
- Jaff MR, McMurtry MS, Archer SL, et al. ; American Heart Association Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation; American Heart Association Council on Peripheral Vascular Disease; American Heart Association Council on Arteriosclerosis, Thrombosis and Vascular Biology . Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Circulation. 2011;123(16):1788-1830. - PubMed
-
- Kaufman JA, Kinney TB, Streiff MB, et al. . Guidelines for the use of retrievable and convertible vena cava filters: report from the Society of Interventional Radiology multidisciplinary consensus conference. J Vasc Interv Radiol. 2006;17(3):449-459. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
