

Temporal Trends and Center Variation in Early Antibiotic Use Among Premature Infants
- PMID: 30646054
- PMCID: PMC6324528
- DOI: 10.1001/jamanetworkopen.2018.0164
Temporal Trends and Center Variation in Early Antibiotic Use Among Premature Infants
Abstract
Importance: Premature infants are frequently administered empirical antibiotic therapy at birth. Early and prolonged antibiotic exposures among infants without culture-confirmed infection have been associated with increased risk of adverse outcomes.
Objective: To examine early antibiotic use among premature infants over time and across hospitals in the United States.
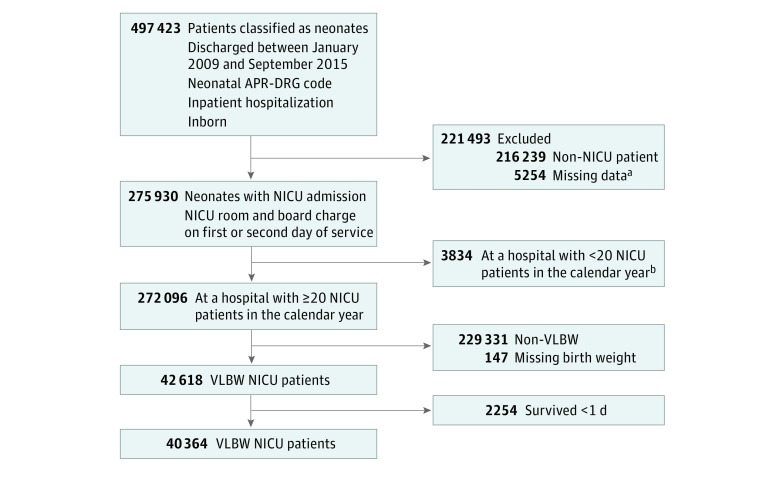
Design, setting, and participants: This retrospective cohort study used a comprehensive administrative database of inpatient encounters from 297 academic and community hospitals across the United States to examine data concerning very low-birth-weight (VLBW) infants (<1500 g), including extremely low-birth-weight (ELBW) infants (<1000 g), who were admitted to the neonatal intensive care unit and survived for at least 1 day. Data collection took place in November 2015 and analysis took place from February 2016 to November 2016.
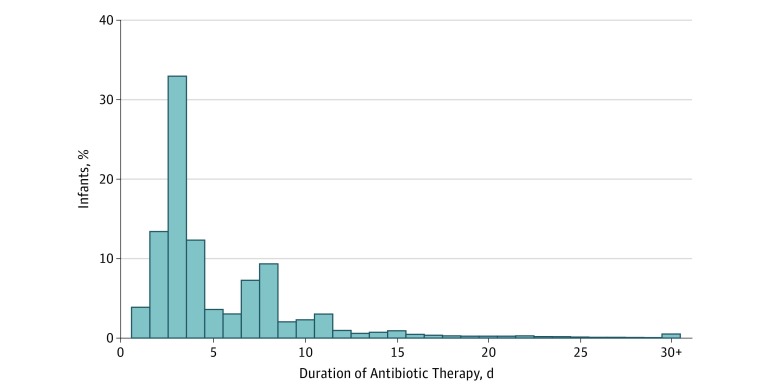
Exposures: Antibiotic initiation within the first 3 days of age and subsequent antibiotic administration for more than 5 days.
Main outcomes and measures: Temporal trends in early antibiotic initiation and duration from 2009 to 2015, and center variation in early antibiotic use from 2014 to 2015.
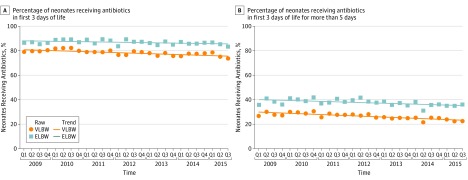
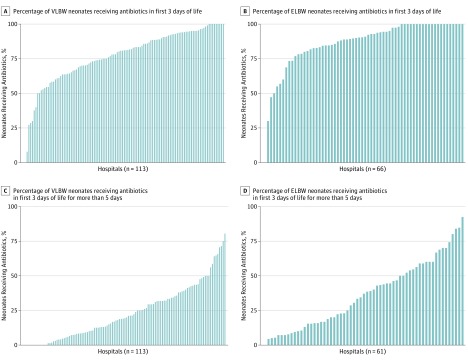
Results: We identified 40 364 VLBW infants (20 447 female [50.7%]) who survived for at least 1 day, including 12 947 ELBW infants, from 297 centers. The majority of premature infants had early antibiotic initiation (31 715 VLBW infants [78.6%] and 11 264 ELBW infants [87.0%]), and no differences were observed over time in temporal trend analyses (P = .12 for VLBW and P = .52 for ELBW). The annual risk difference in the proportion of VLBW infants administered early antibiotic therapy ranged from -0.75% (95% CI, -1.61% to 0.11%) to -0.87% (95% CI, -2.04% to 0.30%); in ELBW infants the annual risk difference ranged from -0.34% (95% CI, -1.28% to 0.61%) to -0.38% (95% CI, -1.61% to 0.85%). There was a small but significant decrease over time in the rate of prolonged antibiotic duration for VLBW infants (P = .02), but not for ELBW infants (P = .22). The annual risk difference in the proportion of VLBW infants with prolonged antibiotic duration ranged from -0.94% (95% CI, -1.65% to -0.23%) to -1.08% (95% CI, -2.00% to -0.16%); in ELBW infants the annual risk difference ranged from -0.72% (95% CI, -1.83% to 0.39%) to -0.75% (95% CI, -1.96% to 0.46%). We also observed variation in early antibiotic exposures across centers. Sixty-nine of 113 centers (61.1%) started antibiotic therapy for more than 75% of VLBW infants, and 56 of 66 centers (84.8%) started antibiotic therapy for more than 75% of ELBW infants. The proportion of VLBW and ELBW infants administered prolonged antibiotics ranged from 0% to 80.4% and 0% to 92.0% across centers, respectively.
Conclusions and relevance: Most premature infants in this study received empirical early antibiotic therapy with little change over a recent 7-year period. The variability in exposure rates across centers, however, suggests that neonatal antimicrobial stewardship efforts are warranted to optimize antibiotic use for VLBW and ELBW infants.
Conflict of interest statement
Figures
Comment in
-
Avoiding Unnecessary Antibiotic Exposure in Premature Infants: Understanding When (Not) to Start and When to Stop.JAMA Netw Open. 2018 May 18;1(1):e180165. doi: 10.1001/jamanetworkopen.2018.0165. JAMA Netw Open. 2018. PMID: 30646051 No abstract available.
References
-
- Grohskopf LA, Huskins WC, Sinkowitz-Cochran RL, Levine GL, Goldmann DA, Jarvis WR; Pediatric Prevention Network . Use of antimicrobial agents in United States neonatal and pediatric intensive care patients. Pediatr Infect Dis J. 2005;24(9):-. - PubMed
-
- Muglia LJ, Katz M. The enigma of spontaneous preterm birth. N Engl J Med. 2010;362(6):529-535. - PubMed
-
- Schrag SJ, Farley MM, Petit S, et al. Epidemiology of invasive early-onset neonatal sepsis, 2005 to 2014. Pediatrics. 2016;138(6):e20162013. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
