

Outpatient Antibiotic Prescribing for Acute Respiratory Infections During Influenza Seasons
- PMID: 30646067
- PMCID: PMC6324415
- DOI: 10.1001/jamanetworkopen.2018.0243
Outpatient Antibiotic Prescribing for Acute Respiratory Infections During Influenza Seasons
Abstract
Importance: Acute respiratory infections (ARIs) are the syndrome for which antibiotics are most commonly prescribed; viruses for which antibiotics are ineffective cause most ARIs.
Objectives: To characterize antibiotic prescribing among outpatients with ARI during influenza season and to identify targets for reducing inappropriate antibiotic prescribing for common ARI diagnoses, including among outpatients with laboratory-confirmed influenza.
Design, setting, and participants: Cohort study enrolling outpatients aged 6 months or older with ARI evaluated at outpatient clinics associated with 5 US Influenza Vaccine Effectiveness Network sites during the 2013-2014 and 2014-2015 influenza seasons. All patients received influenza testing by real-time reverse transcriptase-polymerase chain reaction for research purposes only. Antibiotic prescriptions, medical history, and International Classification of Diseases, Ninth Revision diagnosis codes were collected from medical and pharmacy records, as were group A streptococcal (GAS) testing results in a patient subset.
Exposure: Visit for ARI, defined by a new cough of 7 days' duration or less.
Main outcomes and measures: Antibiotic prescription within 7 days of enrollment. Appropriateness of antibiotic prescribing was based on diagnosis codes, clinical information, and influenza and GAS testing results.
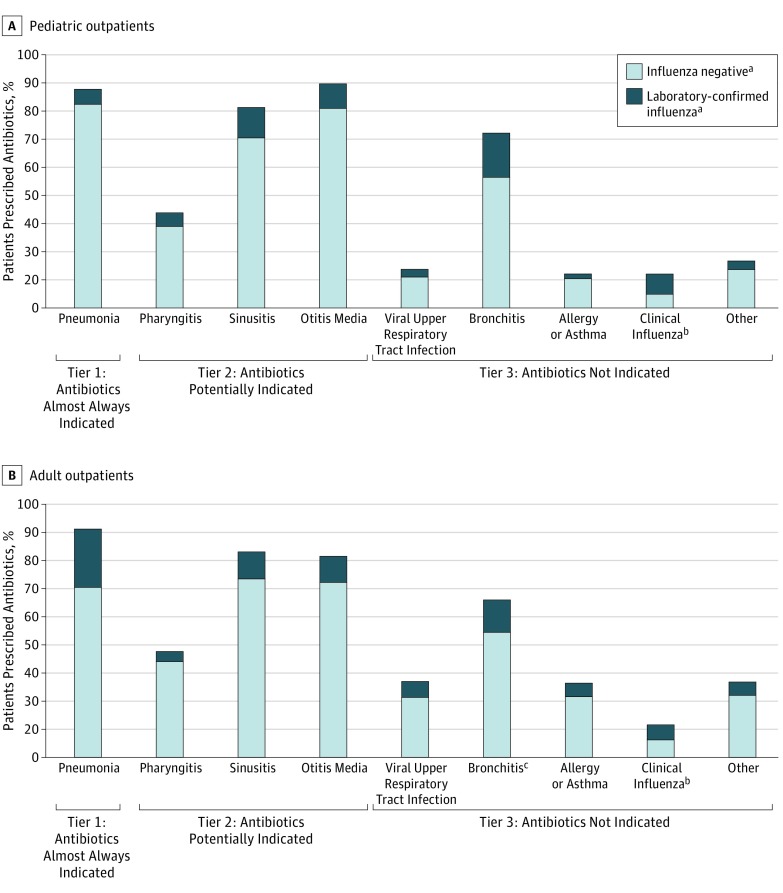
Results: Of 14 987 patients with ARI (mean [SD] age, 32 [24] years; 8638 [58%] women; 11 892 [80%] white), 6136 (41%) were prescribed an antibiotic. Among these 6136 patients, 2522 (41%) had diagnoses for which antibiotics are not indicated; 2106 (84%) of these patients were diagnosed as having a viral upper respiratory tract infection or bronchitis (acute or not otherwise specified). Among the 3306 patients (22%) not diagnosed as having pneumonia and who had laboratory-confirmed influenza, 945 (29%) were prescribed an antibiotic, accounting for 17% of all antibiotic prescriptions among patients with nonpneumonia ARI. Among 1248 patients with pharyngitis, 1137 (91%) had GAS testing; 440 of the 1248 patients (35%) were prescribed antibiotics, among whom 168 (38%) had negative results on GAS testing. Of 1200 patients with sinusitis and no other indication for antibiotic treatment who received an antibiotic, 454 (38%) had symptoms for 3 days or less prior to the outpatient visit, suggesting acute viral sinusitis not requiring antibiotics.
Conclusions and relevance: Antibiotic overuse remains widespread in the treatment of outpatient ARIs, including among patients with laboratory-confirmed influenza, although study sites may not be representative of other outpatient settings. Identified targets for improved outpatient antibiotic stewardship include eliminating antibiotic treatment of viral upper respiratory tract infections and bronchitis and improving adherence to prescribing guidelines for pharyngitis and sinusitis. Increased access to sensitive and timely virus diagnostic tests, particularly for influenza, may reduce unnecessary antibiotic use for these syndromes.
Conflict of interest statement
Figures
References
-
- Centers for Disease Control and Prevention Office-related antibiotic prescribing for persons aged ≤ 14 years—United States, 1993-1994 to 2007-2008. MMWR Morb Mortal Wkly Rep. 2011;60(34):-. - PubMed
-
- Fleming-Dutra KE, Hersh AL, Shapiro DJ, et al. Prevalence of inappropriate antibiotic prescriptions among US ambulatory care visits, 2010-2011. JAMA. 2016;315(17):1864-1873. - PubMed
-
- Centers for Disease Control and Prevention Antibiotic Resistance Threats in the United States, 2013. Atlanta, GA: Centers for Disease Control & Prevention; 2013.
-
- Dooling KL, Shapiro DJ, Van Beneden C, Hersh AL, Hicks LA. Overprescribing and inappropriate antibiotic selection for children with pharyngitis in the United States, 1997-2010. JAMA Pediatr. 2014;168(11):1073-1074. - PubMed
