

Exposure-Response Association Between Concurrent Opioid and Benzodiazepine Use and Risk of Opioid-Related Overdose in Medicare Part D Beneficiaries
- PMID: 30646080
- PMCID: PMC6324417
- DOI: 10.1001/jamanetworkopen.2018.0919
Exposure-Response Association Between Concurrent Opioid and Benzodiazepine Use and Risk of Opioid-Related Overdose in Medicare Part D Beneficiaries
Abstract
Importance: Concurrent benzodiazepine use is associated with an increased risk of opioid-related overdose; however, it remains unknown how the overdose risk varies with the days of exposure to both medications.
Objective: To evaluate the exposure-response association between the days with concurrent prescription opioid and benzodiazepine use and the risk of overdose.
Design, setting, and participants: Retrospective cohort study of Medicare Part D claims data from January 1, 2013, to December 31, 2014. Analyses were conducted in fall 2017 and spring 2018. Participants were Medicare Part D beneficiaries who filled at least 1 prescription for an opioid in 2014.
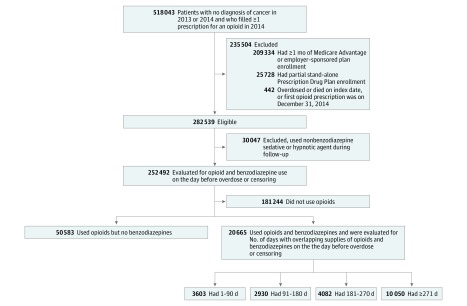
Exposures: Patients were divided into 2 groups based on whether they had opioid and benzodiazepine supplies on the day before overdose or censoring. The first group only had a supply of opioids (n = 50 583) and the second group had supplies of opioids and benzodiazepines (n = 20 665). The second group was further categorized into 4 subgroups based on the cumulative number of days with overlapping supplies of opioids and benzodiazepines: 1 to 90 days (n = 3603), 91 to 180 days (n = 2930), 181 to 270 days (n = 4082), and 271 days or more (n = 10 050).
Main outcomes and measures: Cox proportional hazard models were constructed to compare opioid-related overdose (including fatal and nonfatal overdoses) across time-dependent treatment groups, controlling for demographic characteristics, insurance factors, clinical characteristics, and number of unique opioid and benzodiazepine prescribers.
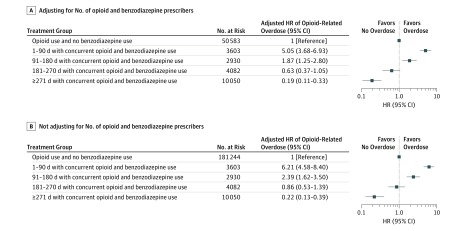
Results: Of 71 248 total participants, 25 600 (35.9%) were male and 59 532 (83.6%) were white. Mean (SD) age was 66.5 (14.8) years. On the day before overdose or censoring event, 20 665 of 71 248 patients with an opioid prescription (29.0%) were concurrently using benzodiazepines and 14 132 of 20 665 concurrent users (68.4%) had more than 180 days of overlapping supplies of both medications. The risk of overdose was highest on the first days of concurrent opioid and benzodiazepine use and decreased over time; compared with opioid use alone, the hazard ratio for overdose was 5.05 (95% CI, 3.68-6.93) during the first 90 days of concurrent opioid and benzodiazepine use and 1.87 (95% CI, 1.25-2.80) for days 91 to 180 among those who did not have an event before 90 days.
Conclusions and relevance: During the first 90 days, concurrent benzodiazepine use is associated with a 5-fold increase in the risk of opioid-related overdose. The implementation of policies deterring concurrent opioid and benzodiazepine use is warranted. Patients using both medications should be closely monitored, particularly during the first days of concurrent use.
Conflict of interest statement
Figures
References
-
- Rudd RA, Seth P, David F, Scholl L. Increases in drug and opioid-involved overdose deaths—United States, 2010-2015. MMWR Morb Mortal Wkly Rep. 2016;65(5051):1445-1452. - PubMed
-
- Crawford C. FDA requires new warnings on combined opioid, benzodiazepine use. American Academy of Family Physicians. http://www.aafp.org/news/health-of-the-public/20160907opioid-benzos.html. Published September 7, 2016. Accessed November 15, 2017.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
