

Risk Factors Associated With Major Cardiovascular Events 1 Year After Acute Myocardial Infarction
- PMID: 30646102
- PMCID: PMC6324290
- DOI: 10.1001/jamanetworkopen.2018.1079
Risk Factors Associated With Major Cardiovascular Events 1 Year After Acute Myocardial Infarction
Abstract
Importance: Patients who survive acute myocardial infarction (AMI) have a high risk of subsequent major cardiovascular events. Efforts to identify risk factors for recurrence have primarily focused on the period immediately following AMI admission.
Objectives: To identify risk factors and develop and evaluate a risk model that predicts 1-year cardiovascular events after AMI.
Design, setting, and participants: Prospective cohort study. Patients with AMI (n = 4227), aged 18 years or older, discharged alive from 53 acute-care hospitals across China from January 1, 2013, to July 17, 2014. Patients were randomly divided into samples: training (50% [2113 patients]), test (25% [1057 patients]), and validation (25% [1057 patients]). Risk factors were identified by a Cox model with Markov chain Monte Carlo simulation and further evaluated by latent class analysis. Analyses were conducted from May 1, 2017, to January 21, 2018.
Main outcomes and measures: Major cardiovascular events, including recurrent AMI, stroke, heart failure, and death, within 1 year after discharge for the index AMI hospitalization.
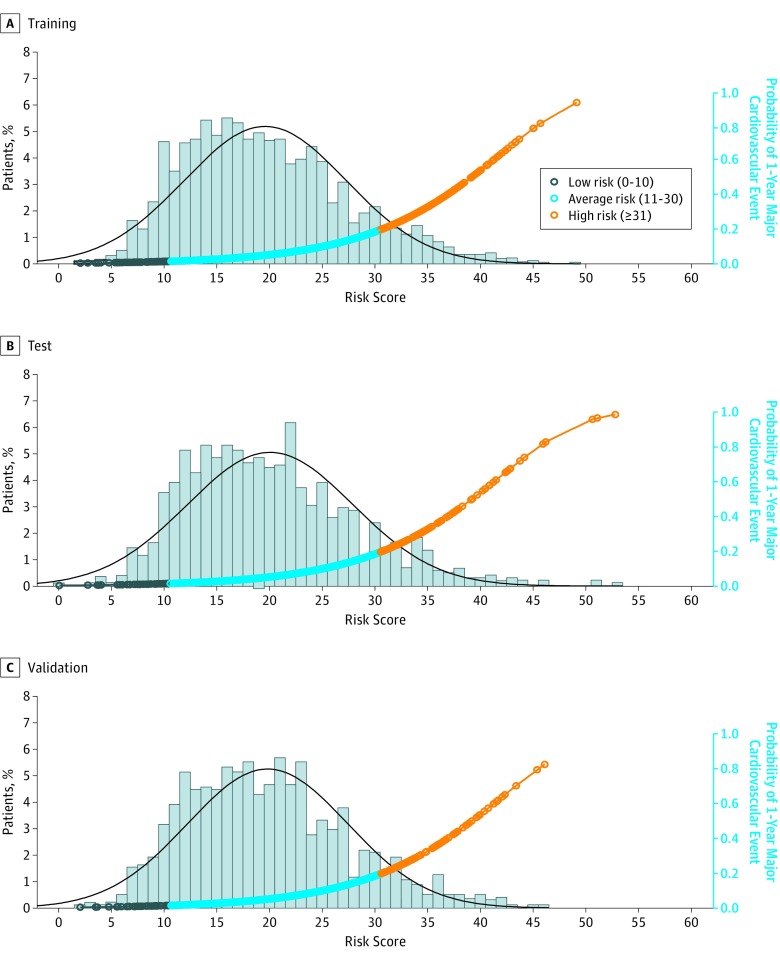
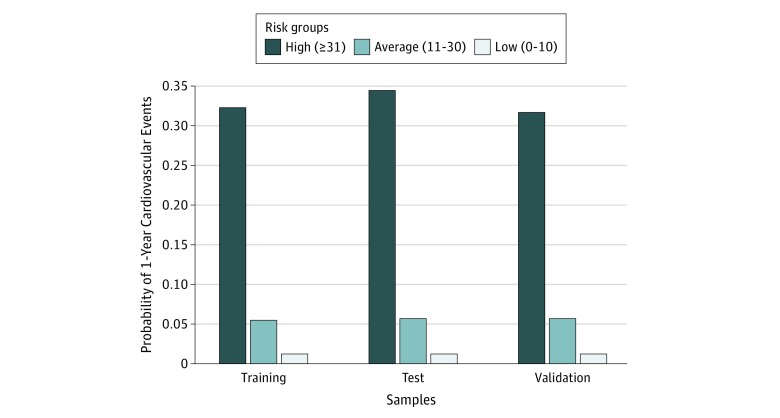
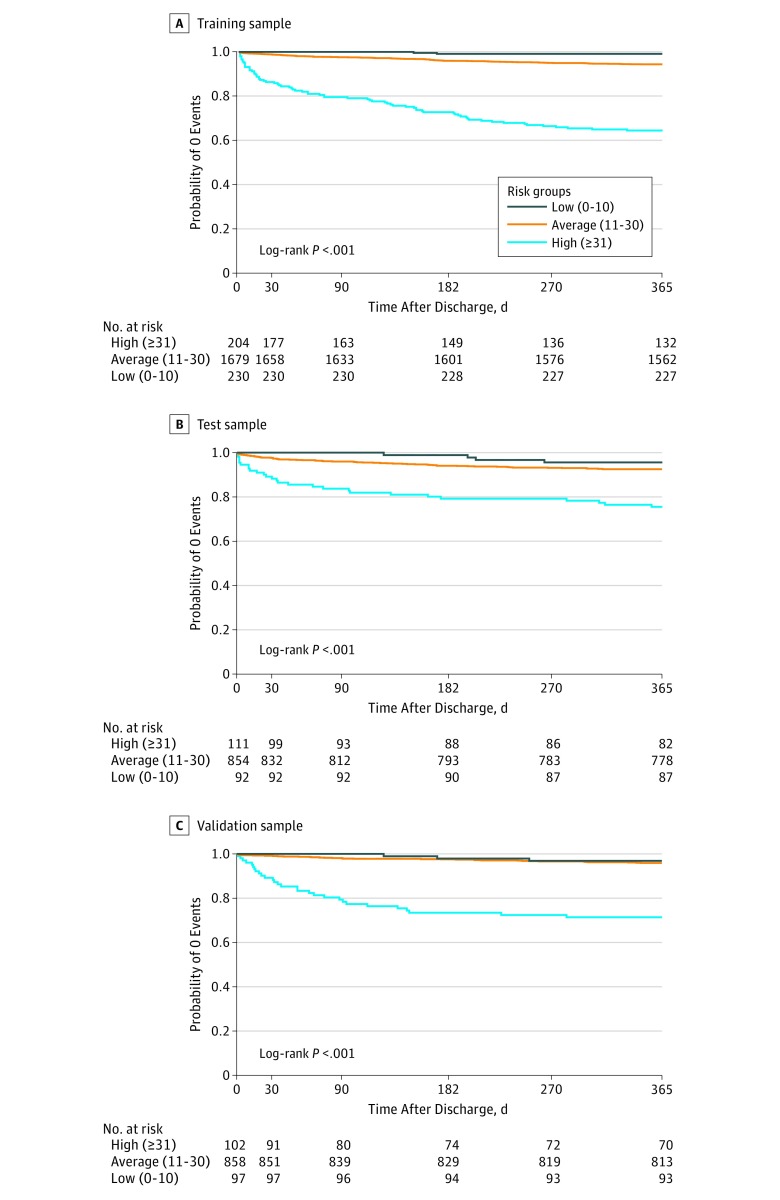
Results: The mean (SD) age of the cohort was 60.8 (11.8) years and 994 of 4227 patients (23.5%) were female. Common comorbidities included hypertension (2358 patients [55.8%]), coronary heart disease (1798 patients [42.5%]), and dyslipidemia (1290 patients [30.5%]). One-year event rates were 8.1% (95% CI, 6.91%-9.24%), 9.0% (95% CI, 7.22%-10.70%), and 6.4% (95% CI, 4.89%-7.85%) for the training, test, and validation samples, respectively. Nineteen risk factors comprising 15 unique variables (age, education, prior AMI, prior ventricular tachycardia or fibrillation, hypertension, angina, prearrival medical assistance, >4 hours from onset of symptoms to admission, ejection fraction, renal dysfunction, heart rate, systolic blood pressure, white blood cell count, blood glucose, and in-hospital complications) were identified. In the training, test, and validation samples, respectively, the risk model had C statistics of 0.79 (95% CI, 0.75-0.83), 0.73 (95% CI, 0.68-0.78), and 0.77 (95% CI, 0.70-0.83) and a predictive range of 1.2% to 33.9%, 1.2% to 37.9%, and 1.3% to 34.3%. The C statistic was 0.69 (95% CI, 0.65-0.74) for the latent class model in the training data. The risk model stratified 11.3%, 81.0%, and 7.7% of patients to high-, average-, and low-risk groups, with respective probabilities of 0.32, 0.06, and 0.01 for 1-year events.
Conclusions and relevance: Nineteen risk factors were identified, and a model was developed and evaluated to predict risk of 1-year cardiovascular events after AMI. This may aid clinicians in identifying high-risk patients who would benefit most from intensive follow-up and aggressive risk factor reduction.
Conflict of interest statement
Figures
References
-
- Smolderen KG, Buchanan DM, Gosch K, et al. . Depression treatment and 1-year mortality following acute myocardial infarction: insights from the TRIUMPH registry (Translational Research Investigating Underlying Disparities in Acute Myocardial Infarction Patients’ Health Status). Circulation. 2017;135(18):1681-1689. doi:10.1161/CIRCULATIONAHA.116.025140 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
