

Exome Sequencing-Based Screening for BRCA1/2 Expected Pathogenic Variants Among Adult Biobank Participants
- PMID: 30646163
- PMCID: PMC6324494
- DOI: 10.1001/jamanetworkopen.2018.2140
Exome Sequencing-Based Screening for BRCA1/2 Expected Pathogenic Variants Among Adult Biobank Participants
Abstract
Importance: Detection of disease-associated variants in the BRCA1 and BRCA2 (BRCA1/2) genes allows for cancer prevention and early diagnosis in high-risk individuals.
Objectives: To identify pathogenic and likely pathogenic (P/LP) BRCA1/2 variants in an unselected research cohort, and to characterize the features associated with P/LP variants.
Design, setting, and participants: This is a cross-sectional study of adult volunteers (n = 50 726) who underwent exome sequencing at a single health care system (Geisinger Health System, Danville, Pennsylvania) from January 1, 2014, to March 1, 2016. Participants are part of the DiscovEHR cohort and were identified through the Geisinger MyCode Community Health Initiative. They consented to a research protocol that included sequencing and return of actionable test results. Clinical data from electronic health records and clinical visits were correlated with variants. Comparisons were made between those with (cases) and those without (controls) P/LP variants in BRCA1/2.
Main outcomes: Prevalence of P/LP BRCA1/2 variants in cohort, proportion of variant carriers not previously ascertained through clinical testing, and personal and family history of relevant cancers among BRCA1/2 variant carriers and noncarriers.
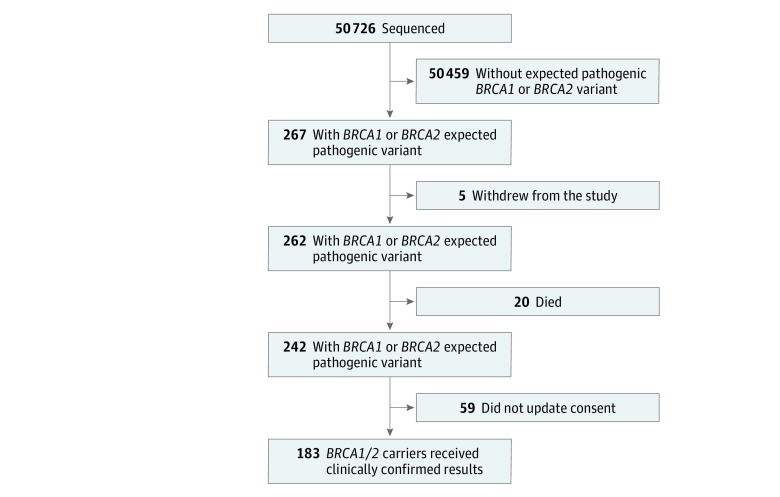
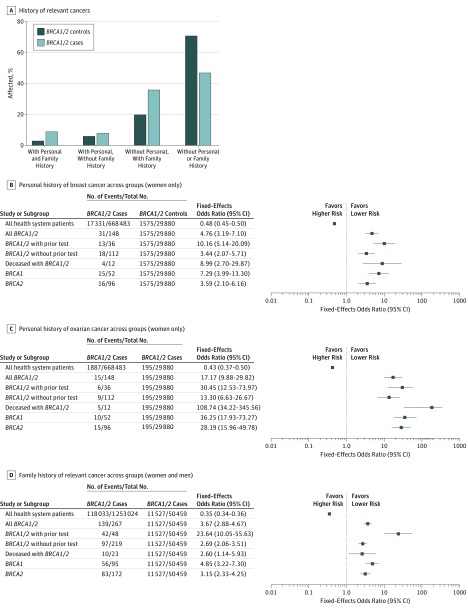
Results: Of the 50 726 health system patients who underwent exome sequencing, 50 459 (99.5%) had no expected pathogenic BRCA1/2 variants and 267 (0.5%) were BRCA1/2 carriers. Of the 267 cases (148 [55.4%] were women and 119 [44.6%] were men with a mean [range] age of 58.9 [23-90] years), 183 (68.5%) received clinically confirmed results in their electronic health record. Among the 267 participants with P/LP BRCA1/2 variants, 219 (82.0%) had no prior clinical testing, 95 (35.6%) had BRCA1 variants, and 172 (64.4%) had BRCA2 variants. Syndromic cancer diagnoses were present in 11 (47.8%) of the 23 deceased BRCA1/2 carriers and in 56 (20.9%) of all 267 BRCA1/2 carriers. Among women, 31 (20.9%) of 148 variant carriers had a personal history of breast cancer, compared with 1554 (5.2%) of 29 880 noncarriers (odds ratio [OR], 5.95; 95% CI, 3.88-9.13; P < .001). Ovarian cancer history was present in 15 (10.1%) of 148 variant carriers and in 195 (0.6%) of 29 880 variant noncarriers (OR, 18.30; 95% CI, 10.48-31.4; P < .001). Among 89 BRCA1/2 carriers without prior testing but with comprehensive personal and family history data, 44 (49.4%) did not meet published guidelines for clinical testing.
Conclusions and relevance: This study found that compared with previous clinical care, exome sequencing-based screening identified 5 times as many individuals with P/LP BRCA1/2 variants. These findings suggest that genomic screening may identify BRCA1/2-associated cancer risk that might otherwise remain undetected within health care systems and may provide opportunities to reduce morbidity and mortality in patients.
Conflict of interest statement
Figures
References
-
- Petrucelli N, Daly MB, Pal T. BRCA1- and BRCA2-associated hereditary breast and ovarian cancer In: Pagon RA, Adam MP, Ardinger HH, et al. , eds. GeneReviews(R). Seattle: University of Washington; 1998. https://www.ncbi.nlm.nih.gov/books/NBK1247/. Updated December 15, 2016. Accessed June 30, 2017. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
