

Association Between Time to Defibrillation and Survival in Pediatric In-Hospital Cardiac Arrest With a First Documented Shockable Rhythm
- PMID: 30646171
- PMCID: PMC6324599
- DOI: 10.1001/jamanetworkopen.2018.2643
Association Between Time to Defibrillation and Survival in Pediatric In-Hospital Cardiac Arrest With a First Documented Shockable Rhythm
Erratum in
-
Error in Key Points.JAMA Netw Open. 2018 Oct 5;1(6):e184644. doi: 10.1001/jamanetworkopen.2018.4644. JAMA Netw Open. 2018. PMID: 30646243 Free PMC article. No abstract available.
Abstract
Importance: Delayed defibrillation (>2 minutes) in adult in-hospital cardiac arrest (IHCA) is associated with worse outcomes. Little is known about the timing and outcomes of defibrillation in pediatric IHCA.
Objective: To determine whether time to first defibrillation attempt in pediatric IHCA with a first documented shockable rhythm is associated with survival to hospital discharge.
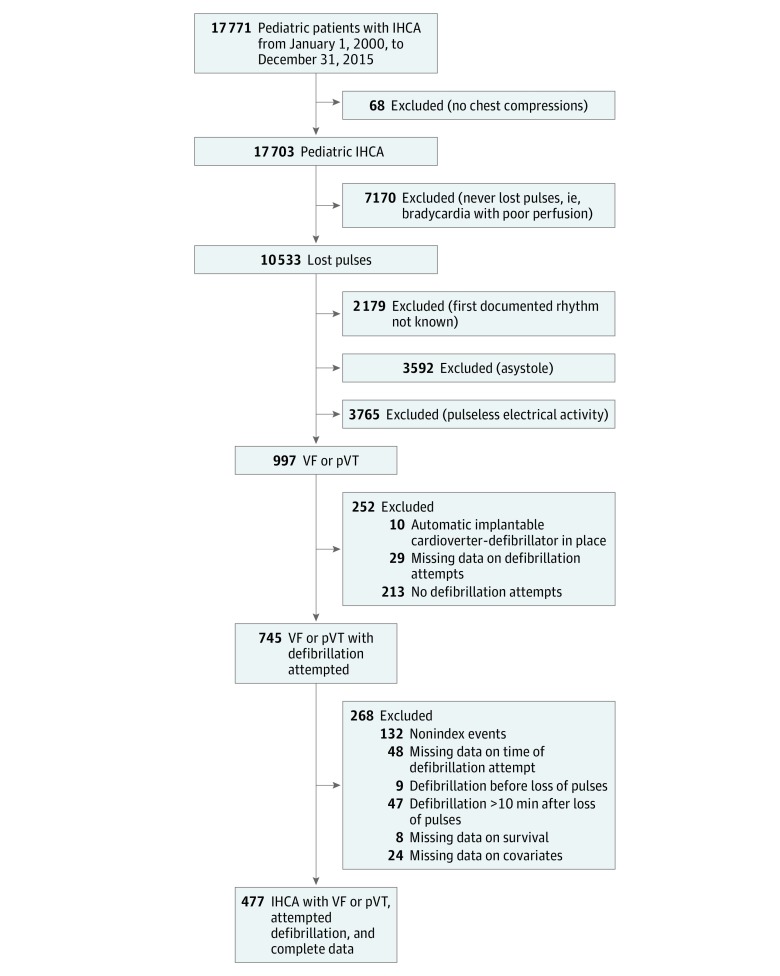
Design, setting, and participants: In this cohort study, data were obtained from the Get With The Guidelines-Resuscitation national registry between January 1, 2000, and December 31, 2015, and analyses were completed by October 1, 2017. Participants were pediatric patients younger than 18 years with an IHCA and a first documented rhythm of pulseless ventricular tachycardia or ventricular fibrillation and at least 1 defibrillation attempt.
Exposures: Time between loss of pulse and first defibrillation attempt.
Main outcomes and measures: The primary outcome was survival to hospital discharge. Secondary outcomes were return of circulation, 24-hour survival, and favorable neurologic outcome at hospital discharge.
Results: Among 477 patients with a pulseless shockable rhythm (median [interquartile range] age, 4 years [3 months to 14 years]; 285 [60%] male), 338 (71%) had a first defibrillation attempt at 2 minutes or less after pulselessness. Children were less likely to be shocked in 2 minutes or less for ward vs intensive care unit IHCAs (48% [11 of 23] vs 72% [268 of 371]; P = .01]). Thirty-eight percent (179 patients) survived to hospital discharge. The median (interquartile range) reported time to first defibrillation attempt was 1 minute (0-3 minutes) in both survivors and nonsurvivors. Time to first defibrillation attempt was not associated with survival in unadjusted analysis (risk ratio [RR] per minute increase, 0.96; 95% CI, 0.92-1.01; P = .15) or adjusted analysis (RR, 0.99; 95% CI, 0.94-1.06; P = .86). There was no difference in survival between those with a first defibrillation attempt in 2 minutes or less vs more than 2 minutes in unadjusted analysis (132 of 338 [39%] vs 47 of 139 [34%]; RR, 0.87; 95% CI, 0.66-1.13; P = .29) or multivariable analysis (RR, 0.99; 95% CI, 0.75-1.30; P = .93). Time to first defibrillation attempt was also not associated with secondary outcome measures.
Conclusions and relevance: In contrast to published adult IHCA and pediatric out-of-hospital cardiac arrest data, no significant association was observed between time to first defibrillation attempt in pediatric IHCA with a first documented shockable rhythm and survival to hospital discharge.
Conflict of interest statement
Figures


Comment in
-
Shorter Time to Defibrillation in Pediatric CPR: Children Are Not Small Adults, but Shock Them Like They Are.JAMA Netw Open. 2018 Sep 7;1(5):e182653. doi: 10.1001/jamanetworkopen.2018.2653. JAMA Netw Open. 2018. PMID: 30646162 No abstract available.
References
-
- Morrison LJ, Neumar RW, Zimmerman JL, et al. ; American Heart Association Emergency Cardiovascular Care Committee, Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation, Council on Cardiovascular and Stroke Nursing, Council on Clinical Cardiology, and Council on Peripheral Vascular Disease . Strategies for improving survival after in-hospital cardiac arrest in the United States: 2013 consensus recommendations: a consensus statement from the American Heart Association. Circulation. 2013;127(14):1538-1563. doi:10.1161/CIR.0b013e31828b2770 - DOI - PubMed
-
- Cheng A, Brown LL, Duff JP, et al. ; International Network for Simulation-Based Pediatric Innovation, Research, & Education (INSPIRE) CPR Investigators . Improving cardiopulmonary resuscitation with a CPR feedback device and refresher simulations (CPR CARES Study): a randomized clinical trial. JAMA Pediatr. 2015;169(2):137-144. doi:10.1001/jamapediatrics.2014.2616 - DOI - PubMed
