

Association of the Hospital Readmissions Reduction Program With Mortality During and After Hospitalization for Acute Myocardial Infarction, Heart Failure, and Pneumonia
- PMID: 30646181
- PMCID: PMC6324473
- DOI: 10.1001/jamanetworkopen.2018.2777
Association of the Hospital Readmissions Reduction Program With Mortality During and After Hospitalization for Acute Myocardial Infarction, Heart Failure, and Pneumonia
Abstract
Importance: The US Hospital Readmissions Reduction Program (HRRP) was associated with reduced readmissions among Medicare beneficiaries hospitalized for acute myocardial infarction (AMI), heart failure (HF), and pneumonia. It is important to assess whether there has been a signal for concomitant harm with an increase in mortality.
Objective: To evaluate whether the announcement or the implementation of HRRP was associated with an increase in either in-hospital or 30-day postdischarge mortality following hospitalization for AMI, HF, or pneumonia.
Design, setting, and participants: In this cohort study, using Medicare data, all hospitalizations for AMI, HF, and pneumonia were identified among fee-for-service Medicare beneficiaries aged 65 years and older from January 1, 2006, to December 31, 2014. These were assessed for changes in trends for risk-adjusted rates of in-hospital and 30-day postdischarge mortality after announcement and implementation of the HRRP using an interrupted time series framework. Analyses were done in November 2017 and December 2017.
Exposures: Announcement of the HRRP in March 2010, and implementation of its penalties in October 2012.
Main outcomes and measures: Monthly risk-adjusted rates of in-hospital and 30-day postdischarge mortality.
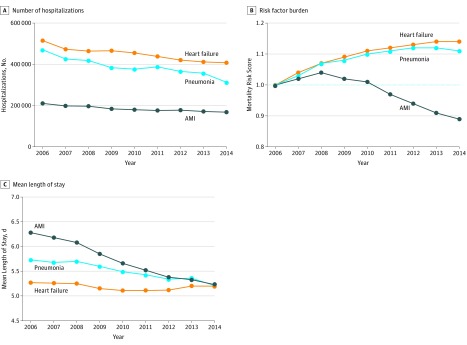
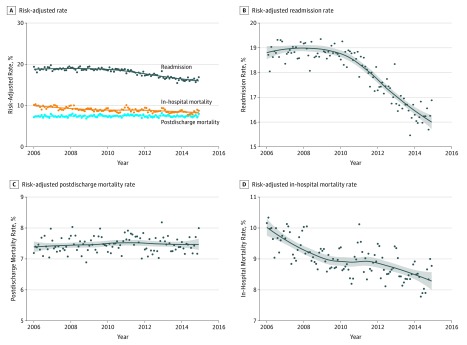
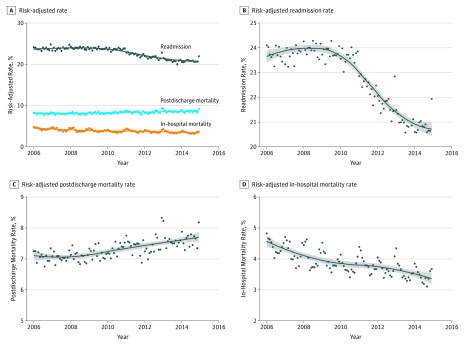
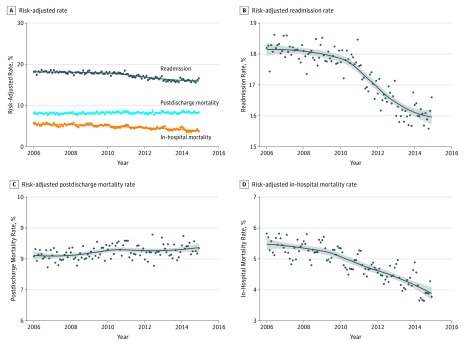
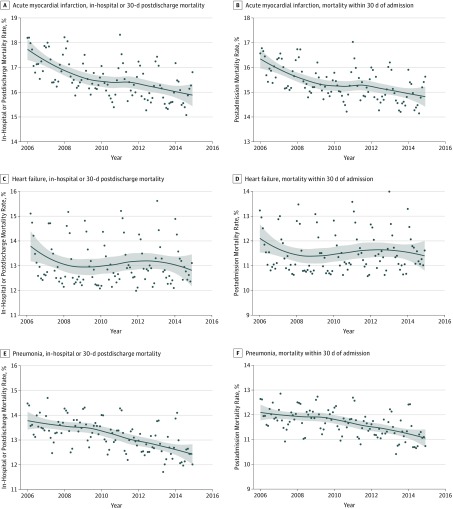
Results: The sample included 1.7 million AMI, 4 million HF, and 3.5 million pneumonia hospitalizations. Between 2006 and 2014, in-hospital mortality decreased for the 3 conditions (AMI, from 10.4% to 9.7%; HF, from 4.3% to 3.5%; pneumonia, from 5.3% to 4.0%) while 30-day postdischarge mortality decreased from 7.4% to 7.0% for AMI (P for trend < .001), but increased from 7.4% to 9.2% for HF (P for trend < .001) and from 7.6% to 8.6% for pneumonia (P for trend < .001). Before the HRRP announcement, monthly postdischarge mortality was stable for AMI (slope for monthly change, 0.002%; 95% CI, -0.001% to 0.006% per month), and increased by 0.004% (95% CI, 0.000% to 0.007%) per month for HF and by 0.005% (95% CI, 0.002% to 0.008%) per month for pneumonia. There were no inflections in slope around HRRP announcement or implementation (P > .05 for all). In contrast, there were significant negative deflections in slopes for readmission rates at HRRP announcement for all conditions.
Conclusions and relevance: Among Medicare beneficiaries, there was no evidence for an increase in in-hospital or postdischarge mortality associated with HRRP announcement or implementation-a period with substantial reductions in readmissions. The improvement in readmission was therefore not associated with any increase in in-hospital or 30-day postdischarge mortality.
Conflict of interest statement
Figures
Comment in
-
Death, Readmissions, and Getting Policy Right.JAMA Netw Open. 2018 Sep 7;1(5):e182776. doi: 10.1001/jamanetworkopen.2018.2776. JAMA Netw Open. 2018. PMID: 30646175 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
