

Association of Embolic Sources With Cause-Specific Functional Outcomes Among Adults With Cryptogenic Stroke
- PMID: 30646186
- PMCID: PMC6324510
- DOI: 10.1001/jamanetworkopen.2018.2953
Association of Embolic Sources With Cause-Specific Functional Outcomes Among Adults With Cryptogenic Stroke
Abstract
Importance: It is unknown whether poststroke outcome varies between different potential causes in patients with cryptogenic stroke.
Objective: To investigate whether functional outcome differs according to potential embolic sources after cryptogenic stroke.
Design, setting, and participants: This multicenter, hospital-based, prospective stroke registry cohort study investigated potential embolic sources on admission and assessed 3-month outcome in patients with ischemic stroke hospitalized at 7 stroke centers in the Fukuoka Stroke Registry. This registry enlisted 9866 consecutive patients with acute ischemic stroke who were enrolled from June 11, 2007, to May 31, 2016, in Fukuoka, Japan. Patients with small vessel occlusion (n = 3130), extracranial and intracranial atherosclerosis causing at least 50% luminal stenosis in arteries supplying the area of ischemia (n = 2011), and other specific uncommon causes of stroke identified (n = 301) were excluded. Potential embolic sources were diagnosed in patients with embolic stroke of undetermined source (ESUS) based on the following criteria proposed by the Cryptogenic Stroke/ESUS International Working Group: minor-risk potential cardioembolic sources (MCS) (n = 209), covert paroxysmal atrial fibrillation (CPAF) (n = 43), cancer associated (CA) (n = 79), arteriogenic emboli (AE) (n = 522), paradoxical embolism (PE) (n = 190), and undetermined embolism (unidentified or ≥2 potential embolic sources) (UE) (n = 1120).
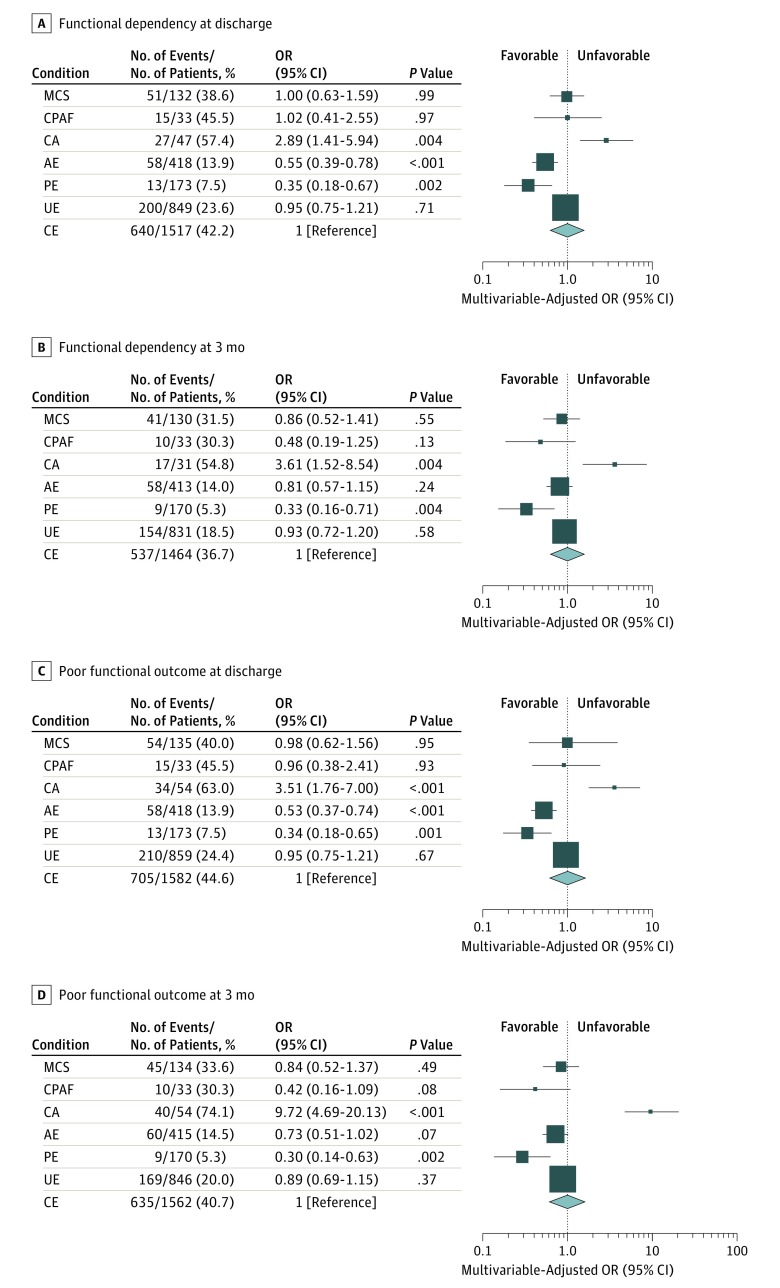
Main outcomes and measures: The association between potential causes and functional outcome was evaluated in reference to cardioembolic stroke (CE) caused by major-risk cardioembolic sources after adjusting for age, sex, National Institutes of Health Stroke Scale score on admission, and reperfusion therapy using logistic regression analysis. Functional dependency (modified Rankin Scale score, 3-5) was evaluated at 3 months after onset.
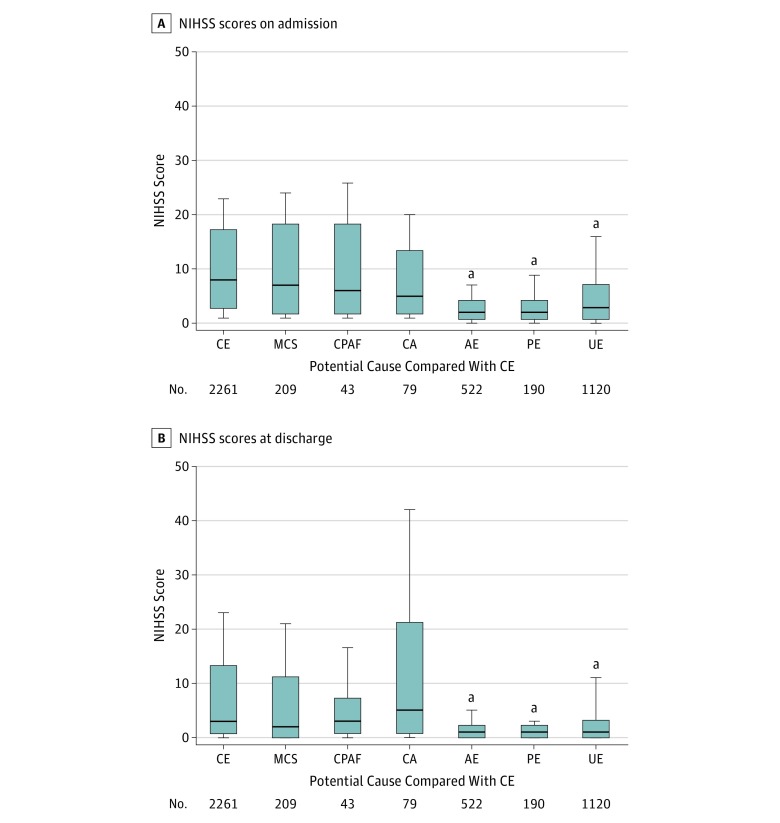
Results: The study enrolled 2261 patients with CE (mean [SD] age, 78.4 [10.7] years, 51.8% male) and 2163 patients with ESUS (mean [SD] age, 72.4 [12.6] years, 57.1% male). Compared with CE (median National Institutes of Health Stroke Scale score, 8 [interquartile range {IQR}, 3-17]), baseline neurological deficits did not differ in MCS (median, 7 [IQR, 2-18]), CPAF (median, 6 [IQR, 2-18]), and CA (median, 5 [IQR, 2-13]) but were less severe in AE (median, 2 [IQR, 1-4]), PE (median, 2 [IQR, 1-4]), and UE (median, 3 [IQR, 1-7]). Multivariable-adjusted odds ratios of functional dependency significantly increased in CA (3.61; 95% CI, 1.52-8.54 vs CE) but decreased in PE (0.33; 95% CI, 0.16-0.71 vs CE).
Conclusions and relevance: Potential causes are associated with poststroke outcome in patients with cryptogenic stroke. Embolic sources potentially underlying cryptogenic stroke should be considered significant variables associated with outcome.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
