

Coverage of Nonpharmacologic Treatments for Low Back Pain Among US Public and Private Insurers
- PMID: 30646222
- PMCID: PMC6324451
- DOI: 10.1001/jamanetworkopen.2018.3044
Coverage of Nonpharmacologic Treatments for Low Back Pain Among US Public and Private Insurers
Abstract
Importance: Despite epidemic rates of addiction and death from prescription opioids in the United States, suggesting the importance of providing alternatives to opioids in the treatment of pain, little is known regarding how payers' coverage policies may facilitate or impede access to such treatments.
Objective: To examine coverage policies for 5 nonpharmacologic approaches commonly used to treat acute or chronic low back pain among commercial and Medicare Advantage insurance plans, plus an additional 6 treatments among Medicaid plans.
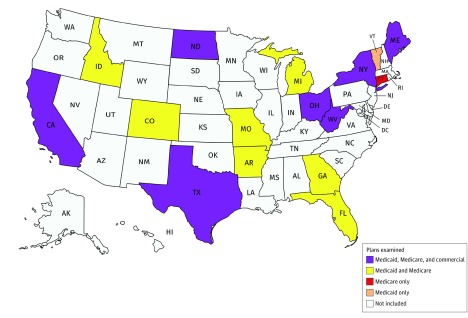
Design, setting, and participants: Cross-sectional study of 15 commercial, 15 Medicaid, and 15 Medicare Advantage health plans for the 2017 calendar year in 16 states representing more than half of the US population. Interviews were conducted with 43 senior medical and pharmacy health plan executives from representative plans.
Main outcomes and measures: Medical necessity and coverage status for the treatments examined, as well as the use of utilization management tools and cost-sharing magnitude and structure.
Results: Commercial and Medicare insurers consistently regarded physical and occupational therapy as medically necessary, but policies varied for other therapies examined. Payers most commonly covered physical therapy (98% [44 of 45 plans]), occupational therapy (96% [43 of 45 plans]), and chiropractic care (89% [40 of 45 plans]), while transcutaneous electrical nerve stimulation (67% [10 of 15 plans]) and steroid injections (60% [9 of 15 plans]) were the most commonly covered among the therapies examined for Medicaid plans only. Despite evidence in the literature to support use of acupuncture and psychological interventions, these therapies were either not covered by plans examined (67% of all plans [30 of 45] did not cover acupuncture) or lacked information about coverage (80% of Medicaid plans [12 of 15] lacked information about coverage of psychological interventions). Utilization management tools, such as prior authorization, were common, but criteria varied greatly with respect to which conditions and what quantity and duration of services were covered. Interviewees represented 6 Medicaid managed care organizations, 2 Medicare Advantage or Part D plans, 9 commercial plans, and 3 trade organizations (eg, Blue Cross Blue Shield Association). Interviews with plan executives indicated a low level of integration between the coverage decision-making processes for pharmacologic and nonpharmacologic therapies for chronic pain.
Conclusions and relevance: Wide variation in coverage of nonpharmacologic treatments for low back pain may be driven by the absence of best practices, the administrative complexities of developing and revising coverage policies, and payers' economic incentives. Such variation suggests an important opportunity to improve the accessibility of services, reduce opioid use, and ultimately improve the quality of care for individuals with chronic, noncancer pain while alleviating the burden of opioid addiction and overdose.
Conflict of interest statement
Figures
Comment in
-
Insurer Coverage of Nonpharmacological Treatments for Low Back Pain-Time for a Change.JAMA Netw Open. 2018 Oct 5;1(6):e183037. doi: 10.1001/jamanetworkopen.2018.3037. JAMA Netw Open. 2018. PMID: 30646214 No abstract available.
References
-
- Centers for Disease Control and Prevention (CDC) Vital signs: overdoses of prescription opioid pain relievers—United States, 1999-2008. MMWR Morb Mortal Wkly Rep. 2011;60(43):-. - PubMed
-
- Behavioral Health Coordinating Committee, Prescription Drug Abuse Subcommittee Addressing Prescription Drug Abuse in the United States: Current Activities and Future Opportunities Washington, DC: US Department of Health and Human Services; 2013. https://www.cdc.gov/drugoverdose/pdf/hhs_prescription_drug_abuse_report_.... Accessed December 28, 2017.
-
- Hedegaard H, Warner M, Minino AM Drug overdose deaths in the United States, 1999-2016. https://www.cdc.gov/nchs/products/databriefs/db294.htm. Published December 2017. Accessed December 28, 2017.
-
- Center for Behavioral Health Statistics and Quality Key substance use and mental health indicators in the United States: results from the 2015 National Survey on Drug Use and Health. http://www.samhsa.gov/data/. Published 2016. Accessed December 28, 2017.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
