Factors Associated With Cancer Disparities Among Low-, Medium-, and High-Income US Counties
- PMID: 30646225
- PMCID: PMC6324449
- DOI: 10.1001/jamanetworkopen.2018.3146
Factors Associated With Cancer Disparities Among Low-, Medium-, and High-Income US Counties
Abstract
Background: There are concerns about the degree to which county income level might underlie the stark disparities in cancer death rates among US counties; at the same time, there is uncertainty about the factors that may mediate the disparities.
Objectives: To assess county-level cancer death rates and to identify possible mediators of the association between county-level median incomes and cancer death rates.
Design, setting, and participants: Cross-sectional study using death records from the National Center for Health Statistics in 2014, with data collected and analyzed between October 1, 2016, and July 31, 2017. All US counties and county equivalents were included.
Exposures: County-level median household income.
Main outcomes and measures: County-level age-standardized cancer death rate.
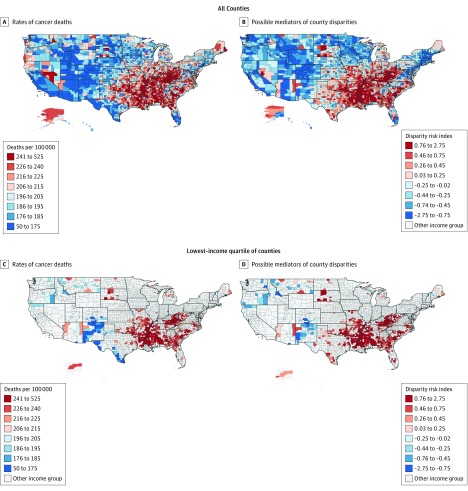
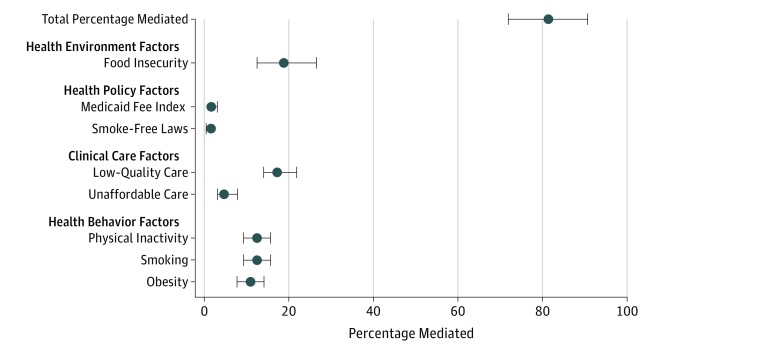
Results: In 3135 counties, median incomes ranged from $22 126 to $121 250 per year. Low-income counties (median income, $33 445) vs high-income counties (median income, $55 780) had higher proportions of residents who were non-Hispanic black, lived in rural areas, or reported poor or fair health. The mean (SD) cancer death rate was 185.9 (24.4) per 100 000 person-years in high-income counties, compared with 204.9 (26.3) and 229.7 (32.9) per 100 000 person-years in medium- and low-income counties, respectively. In mediation models, health risk behaviors (smoking, obesity, and physical inactivity); clinical care factors (unaffordable care and low-quality care); health environments (food insecurity); and health policies (state smoke-free laws and Medicaid payment rates) in aggregate accounted for more than 80% of the income-related disparity. The strongest possible mediators were food insecurity (explaining 19.1% [95% CI, 12.5%-26.5%] of the association between county incomes and cancer deaths), low-quality care (17.9%; 95% CI, 14.0%-21.8%), smoking (12.7%; 95% CI, 9.4%-15.6%), and physical inactivity (12.2%; 95% CI, 9.4%-15.6%).
Conclusions and relevance: There are wide gaps in cancer death rates between low-, medium-, and high-income counties. Future studies are needed to assess whether targeting the possible mediators might ameliorate the substantial socioeconomic cancer disparities.
Conflict of interest statement
Figures