

Outcomes of Hospital Transfers for Pediatric Abdominal Pain and Appendicitis
- PMID: 30646237
- PMCID: PMC6324598
- DOI: 10.1001/jamanetworkopen.2018.3249
Outcomes of Hospital Transfers for Pediatric Abdominal Pain and Appendicitis
Abstract
Importance: Hospital care for children is becoming more concentrated, with interhospital transfer occurring more frequently even for common conditions. Condition-specific analysis is required to determine the value, costs, and consequences of this trend.
Objectives: To describe the capabilities of transferring and receiving hospitals and to determine how often children transferred after an initial diagnosis of abdominal pain or appendicitis require higher levels of care.
Design, setting, and participants: Retrospective cohort analysis using the 2 most recent available inpatient and emergency department administrative data sets from all acute care hospitals in California from 2010 to 2011 and Florida, Massachusetts, and New York from 2013 to 2014. Data were analyzed between February and June 2018. All patients younger than 18 years with a primary diagnosis of abdominal pain or appendicitis who underwent an interhospital transfer and whose care could be matched through unique identifiers were included.
Main outcomes and measures: Outcomes after hospital transfers, classified into encounters with major surgical procedures, imaging diagnostics, and no major procedures. Pediatric Hospital Capability Index of transferring and receiving hospitals.
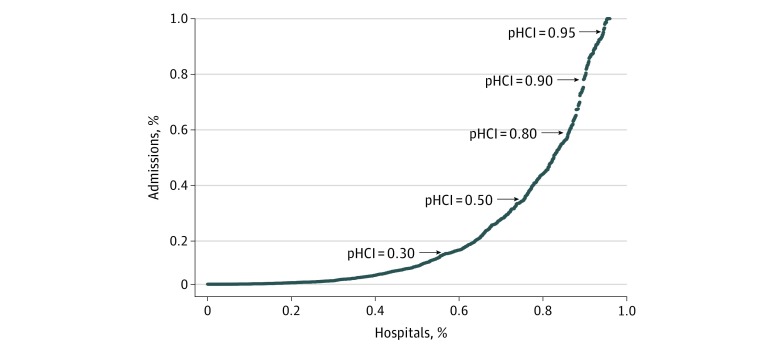
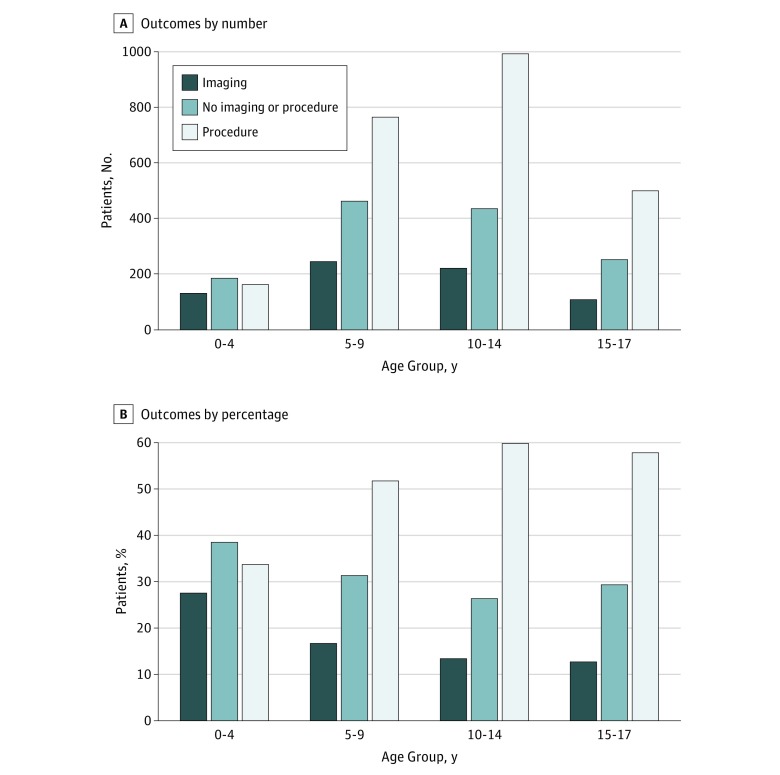
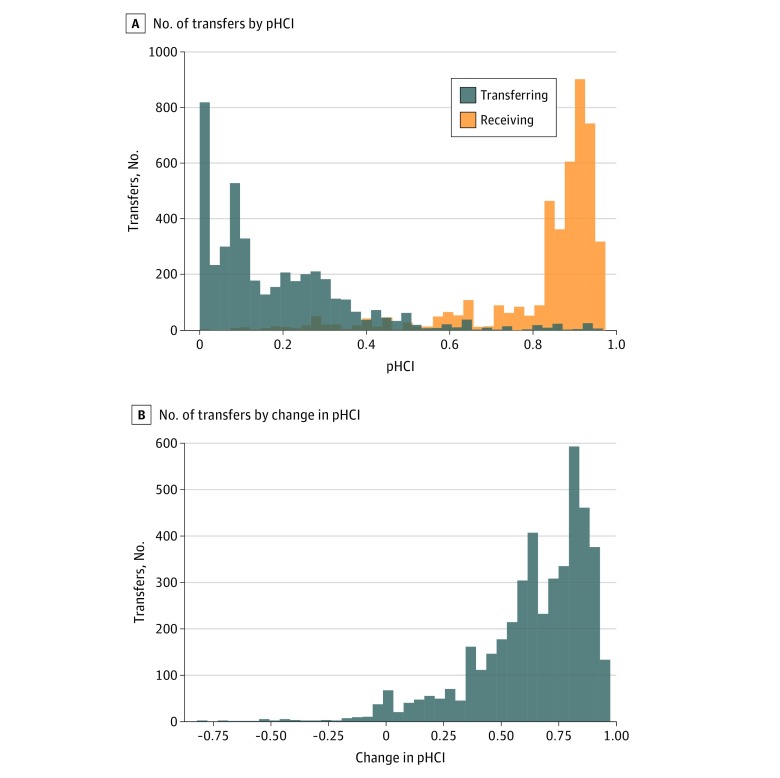
Results: There were 465 143 pediatric hospital encounters for abdominal pain and appendicitis, including 53 517 inpatient admissions and 15 275 transfers. Among them, 4469 could be matched to encounters in receiving hospitals. The median (interquartile range) age of this cohort was 10 (7-14) years, with 54.8% female (2449 patients), 40.9% male (1830 patients), and 4.3% unreported sex (190 patients). The increase in capability at the receiving hospital compared with the transferring hospital was large (median [interquartile range] change in Pediatric Hospital Capability Index score, 0.70 [0.54-0.82]), with 9.2% of hospitals (57) with very high capability (Pediatric Hospital Capability Index score >0.77) receiving 80.8% of the total transfers (3610). Diagnostic imaging was undertaken in the care of 710 transferred patients (15.9%) and invasive procedures were performed in 2421 patients (54.2%), including 2153 appendectomies. No imaging or surgery was required in the care of 1338 transfers (29.9%).
Conclusions and relevance: In this study, interfacility transfers of patients with appendicitis and abdominal pain were concentrated toward high-capability hospitals, and about 30% of patients were released without apparent intervention. These findings suggest an opportunity for improving care and decreasing cost through better interfacility coordination, such as standardized management protocols and telemedicine with high-capability hospitals. Further research is needed to identify similar opportunities among other common conditions.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
