

Association of Cardiorespiratory Fitness With Long-term Mortality Among Adults Undergoing Exercise Treadmill Testing
- PMID: 30646252
- PMCID: PMC6324439
- DOI: 10.1001/jamanetworkopen.2018.3605
Association of Cardiorespiratory Fitness With Long-term Mortality Among Adults Undergoing Exercise Treadmill Testing
Abstract
Importance: Adverse cardiovascular findings associated with habitual vigorous exercise have raised new questions regarding the benefits of exercise and fitness.
Objective: To assess the association of all-cause mortality and cardiorespiratory fitness in patients undergoing exercise treadmill testing.
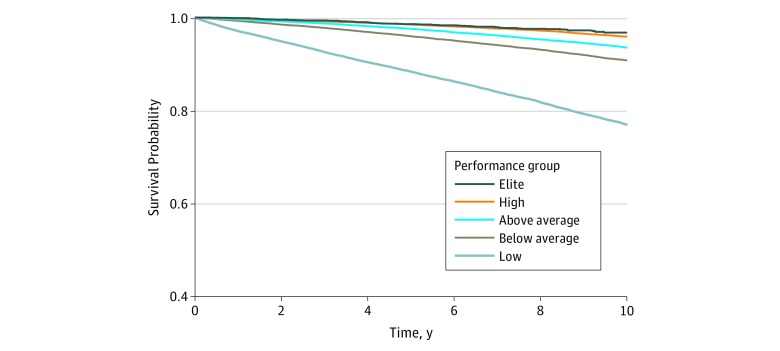
Design, setting, and participants: This retrospective cohort study enrolled patients at a tertiary care academic medical center from January 1, 1991, to December 31, 2014, with a median follow-up of 8.4 years. Data analysis was performed from April 19 to July 17, 2018. Consecutive adult patients referred for symptom-limited exercise treadmill testing were stratified by age- and sex-matched cardiorespiratory fitness into performance groups: low (<25th percentile), below average (25th-49th percentile), above average (50th-74th percentile), high (75th-97.6th percentile), and elite (≥97.7th percentile).
Exposures: Cardiorespiratory fitness, as quantified by peak estimated metabolic equivalents on treadmill testing.
Main outcomes and measures: All-cause mortality.
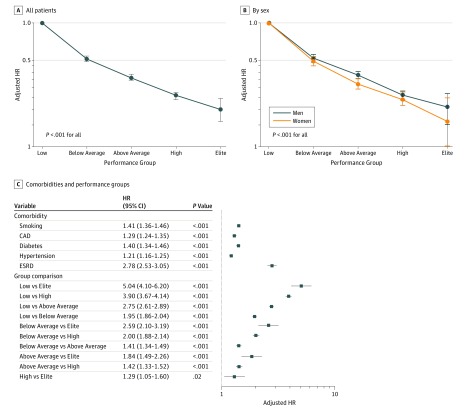
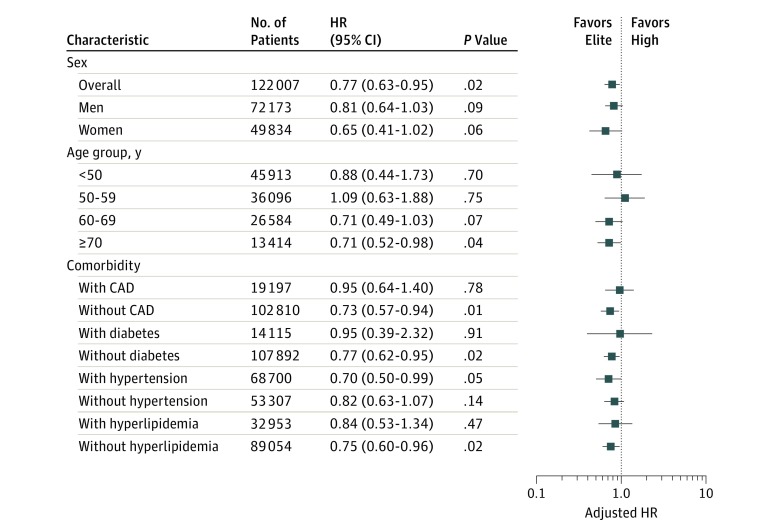
Results: The study population included 122 007 patients (mean [SD] age, 53.4 [12.6] years; 72 173 [59.2%] male). Death occurred in 13 637 patients during 1.1 million person-years of observation. Risk-adjusted all-cause mortality was inversely proportional to cardiorespiratory fitness and was lowest in elite performers (elite vs low: adjusted hazard ratio [HR], 0.20; 95% CI, 0.16-0.24; P < .001; elite vs high: adjusted HR, 0.77; 95% CI, 0.63-0.95; P = .02). The increase in all-cause mortality associated with reduced cardiorespiratory fitness (low vs elite: adjusted HR, 5.04; 95% CI, 4.10-6.20; P < .001; below average vs above average: adjusted HR, 1.41; 95% CI, 1.34-1.49; P < .001) was comparable to or greater than traditional clinical risk factors (coronary artery disease: adjusted HR, 1.29; 95% CI, 1.24-1.35; P < .001; smoking: adjusted HR, 1.41; 95% CI, 1.36-1.46; P < .001; diabetes: adjusted HR, 1.40; 95% CI, 1.34-1.46; P < .001). In subgroup analysis, the benefit of elite over high performance was present in patients 70 years or older (adjusted HR, 0.71; 95% CI, 0.52-0.98; P = .04) and patients with hypertension (adjusted HR, 0.70; 95% CI, 0.50-0.99; P = .05). Extreme cardiorespiratory fitness (≥2 SDs above the mean for age and sex) was associated with the lowest risk-adjusted all-cause mortality compared with all other performance groups.
Conclusions and relevance: Cardiorespiratory fitness is inversely associated with long-term mortality with no observed upper limit of benefit. Extremely high aerobic fitness was associated with the greatest survival and was associated with benefit in older patients and those with hypertension. Cardiorespiratory fitness is a modifiable indicator of long-term mortality, and health care professionals should encourage patients to achieve and maintain high levels of fitness.
Conflict of interest statement
Figures
Comment in
-
Cardiorespiratory Fitness and Physical Activity: Two Important but Distinct Clinical Measures with Different Degrees of Precision - A Commentary.Prog Cardiovasc Dis. 2019 Jan-Feb;62(1):74-75. doi: 10.1016/j.pcad.2018.11.011. Epub 2018 Nov 24. Prog Cardiovasc Dis. 2019. PMID: 30481510 No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
