

Rates of Repeated Operation for Isolated Subdural Hematoma Among Older Adults
- PMID: 30646255
- PMCID: PMC6324600
- DOI: 10.1001/jamanetworkopen.2018.3737
Rates of Repeated Operation for Isolated Subdural Hematoma Among Older Adults
Abstract
Importance: Elderly patients who undergo surgery for an isolated nontraumatic subdural hematoma (SDH) are at major risk for SDH reaccumulation, which can cause further injury and disability. Few population-based studies have examined how often nontraumatic SDH reaccumulates and necessitates repeated operation.
Objective: To determine the rate of repeated operation after evacuation of nontraumatic SDH.
Design, setting, and participants: In a cohort study, 2 parallel analyses were performed using data from the National Surgical Quality Improvement Project (NSQIP) from January 1, 2012, through December 31, 2015, and inpatient and outpatient claims data from a 5% nationally representative sample of Medicare beneficiaries from January 1, 2009, to September 30, 2015. In both samples, our cohort comprised patients 65 years or older who underwent surgical evacuation of nontraumatic SDH. Data were analyzed from March 28 to April 13, 2018.
Main outcomes and measures: The outcome variable was repeated operation for SDH after the index operation. Survival analysis and Kaplan-Meier statistics were used to calculate cumulative rates.
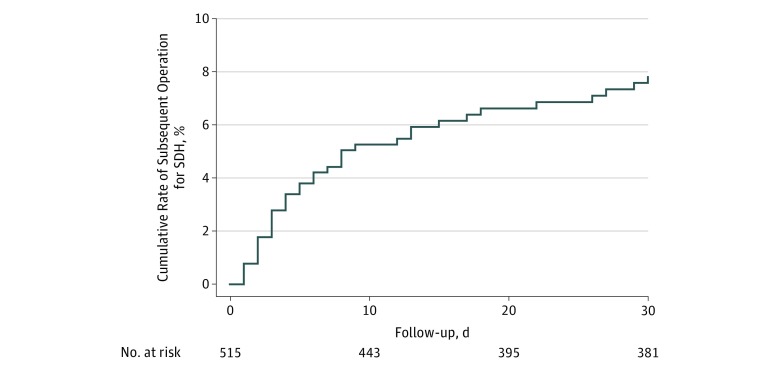
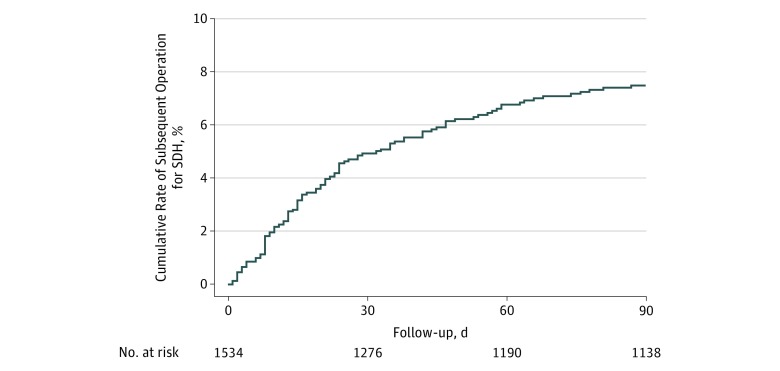
Results: Among 2 831 274 cases submitted to the NSQIP registry, 515 patients 65 years or older (mean [SD] age, 76.9 [7.4] years; 177 [34.4%] women; 367 [71.3%] white) who underwent craniotomy or craniectomy for nontraumatic SDH were identified. Within 30 days after the index surgery, 37 patients underwent a repeated operation for SDH. The cumulative 30-day mortality rate was 13.8% (95% CI, 11.0%-17.1%), and the repeated operation rate was 7.8% (95% CI, 5.7%-10.7%). Among a cohort of 1 952 305 Medicare beneficiaries, 1534 patients (mean [SD] age, 77.7 [7.0] years; 498 [32.5%] women; 1244 [81.1%] white) who underwent evacuation of nontraumatic SDH were identified. A total of 103 patients underwent a repeated operation within 90 days. The cumulative 30-day mortality rate was 11.6% (95% CI, 10.1%-13.3%), and the repeated operation rate was 4.9% (95% CI, 3.9%-6.2%); the cumulative 90-day mortality rate was 17.6% (95% CI, 15.7%-19.6%), and the repeated operation rate was 7.5% (95% CI, 6.2%-9.0%). The study found no evidence of a significant difference in cumulative repeated operation rates at 90 days between patients whose index surgery was a burr-hole procedure for chronic SDH (11.7%; 95% CI, 6.3%-21.3%) vs a craniotomy or craniectomy (7.2%; 95% CI, 6.0%-8.8%) (P = .14 by the log-rank test).
Conclusions and relevance: In 2 large cohorts of US patients, approximately 5% to 10% of patients who underwent surgery for nontraumatic SDH were required to undergo repeated operation within 30 to 90 days. These results may inform the design of future prospective studies and trials and help practitioners calibrate their index of suspicion to ensure that patients are referred for timely surgical care.
Conflict of interest statement
Figures
References
-
- Bullock MR, Chesnut R, Ghajar J, et al. ; Surgical Management of Traumatic Brain Injury Author Group . Surgical management of acute subdural hematomas. Neurosurgery. 2006;58(3)(suppl):S16-S24. - PubMed
-
- Schaumann A, Klene W, Rosenstengel C, Ringel F, Tüttenberg J, Vajkoczy P. COXIBRAIN: results of the prospective, randomised, phase II/III study for the selective COX-2 inhibition in chronic subdural haematoma patients. Acta Neurochir (Wien). 2016;158(11):2039-2044. doi: 10.1007/s00701-016-2949-3 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
