

Effect of 2 Clinical Decision Support Strategies on Chronic Kidney Disease Outcomes in Primary Care: A Cluster Randomized Trial
- PMID: 30646261
- PMCID: PMC6324427
- DOI: 10.1001/jamanetworkopen.2018.3377
Effect of 2 Clinical Decision Support Strategies on Chronic Kidney Disease Outcomes in Primary Care: A Cluster Randomized Trial
Abstract
Importance: Information is needed about optimal strategies to improve evidence-based treatment of chronic kidney disease (CKD) in primary care.
Objective: To determine whether a multimodal intervention delays annualized loss of estimated glomerular filtration rate (eGFR) in stages 3 and 4 CKD.
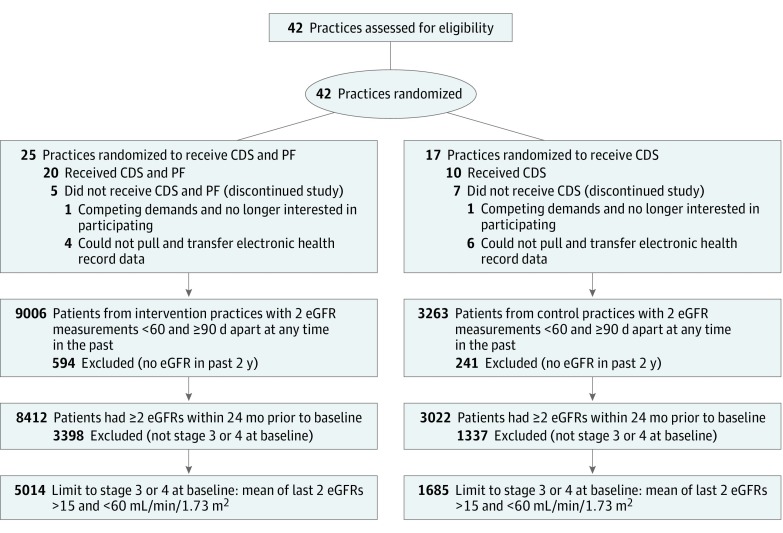
Design, setting, and participants: This pragmatic cluster randomized clinical trial enrolled 42 primary care practices located in nonhospital settings with electronic health record systems. Practices were recruited through the American Academy of Family Physicians National Research Network. The study was conducted January 2013 through January 2016.
Interventions: Practices were randomized at the organization level to either the clinical decision support (CDS) plus practice facilitation (PF) group (n = 25) or CDS group (n = 17) using covariate constrained randomization. Both groups received point-of-care CDS to prompt screening, diagnosis, and treatment of CKD; the intervention group also received PF based on the 9-point TRANSLATE model (target, use point-of-care reminder systems, get administrative buy-in, network information systems using registries, site coordination, local physician champion, audit and feedback, team approach, and education).
Main outcomes and measures: The primary outcome measure was eGFR over time. Secondary outcome measures were systolic blood pressure over time, change in hemoglobin A1c (HbA1c) over time, avoidance of nonsteroidal anti-inflammatory medications, use of angiotensin converting enzyme inhibitor or angiotensin-renin blocker medication, early recognition and diagnosis of CKD, blood pressure control, and smoking cessation.
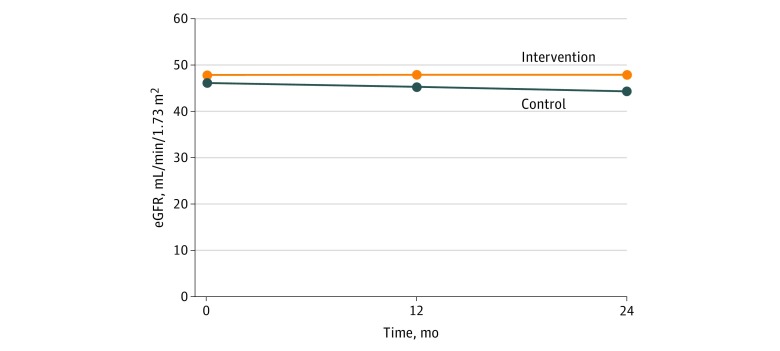
Results: In this cluster randomized trial of 30 primary care practices comprising 6699 patients, there were 1685 patients in the control group (10 practices) and 5014 patients in the intervention group (20 practices). The final sample of practices differed from the original set of randomized practices owing to dropout. Patients in the practices were similar at baseline for age (mean [SD], 71.3 [9.6] years), sex (2716 male [40.5%]), and eGFR. There was a significant difference in eGFR slopes for patients in the intervention vs control group practices. The mean (SE) annualized loss of eGFR was 0.95 (0.19) in the control group in propensity-adjusted longitudinal analyses and 0.01 (0.12) in the intervention group (mean [SE] difference in slopes, 0.93 [0.23]; P < .001). Among patients with HbA1c measures, slopes differed significantly for patients in intervention vs control practices, with a mean (SE) annualized increase of 0.14 (0.03) in HbA1c for patients in control practices and a mean (SE) decline of 0.009 (0.02) for patients in intervention practices. There was a significant difference in HbA1c slopes for patients in the intervention compared with control group practices (control vs intervention, -0.14; P < .001), but no difference in the other secondary outcomes.
Conclusions and relevance: A multimodal intervention in primary care, based on the TRANSLATE model, slowed annualized loss of eGFR. This study had several important strengths, weaknesses, and lessons learned regarding the implementation of pragmatic interventions in primary care to improve CKD outcomes.
Trial registration: ClinicalTrials.gov Identifier: NCT01767883.
Conflict of interest statement
Figures
Comment in
-
The Promise and Pitfalls of Pragmatic Clinical Trials for Improving Health Care Quality.JAMA Netw Open. 2018 Oct 5;1(6):e183376. doi: 10.1001/jamanetworkopen.2018.3376. JAMA Netw Open. 2018. PMID: 30646258 No abstract available.
References
-
- Centers for Disease Control and Prevention Chronic Kidney Disease Surveillance System—United States. Crude prevalence of CKD stages 1-4, 1999-2014. https://nccd.cdc.gov/ckd/detail.aspx?Qnum=Q9. Accessed November 2, 2017.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
