United States State-Level Variation in the Use of Neuraxial Analgesia During Labor for Pregnant Women
- PMID: 30646335
- PMCID: PMC6324365
- DOI: 10.1001/jamanetworkopen.2018.6567
United States State-Level Variation in the Use of Neuraxial Analgesia During Labor for Pregnant Women
Abstract
Importance: Neuraxial labor analgesia is recognized as the most effective method of providing pain relief during labor. Little is known about variation in the rates of neuraxial analgesia across US states. Identifying the presence and extent of variation may provide insights into practice variation and may indicate where access to neuraxial analgesia is inadequate.
Objective: To test the hypothesis that variation exists in neuraxial labor analgesia use among US states.
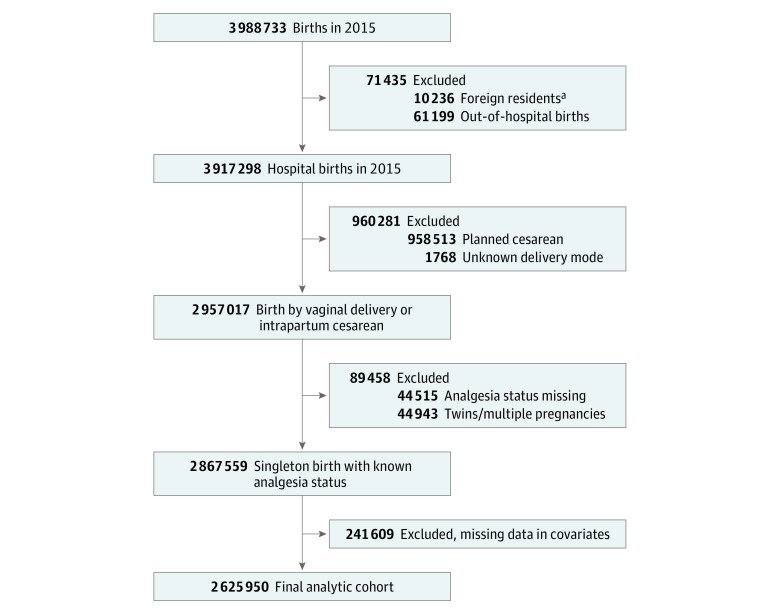
Design, setting, and participants: Retrospective, population-based, cross-sectional analysis using US birth certificate data. Participants were 2 625 950 women who underwent labor in 2015.
Main outcomes and measures: State-specific prevalence of neuraxial analgesia per 100 women who underwent labor and variability in neuraxial analgesia use among states, assessed using multilevel multivariable regression modeling with the median odds ratio and the intraclass correlation coefficient to evaluate variation by state.
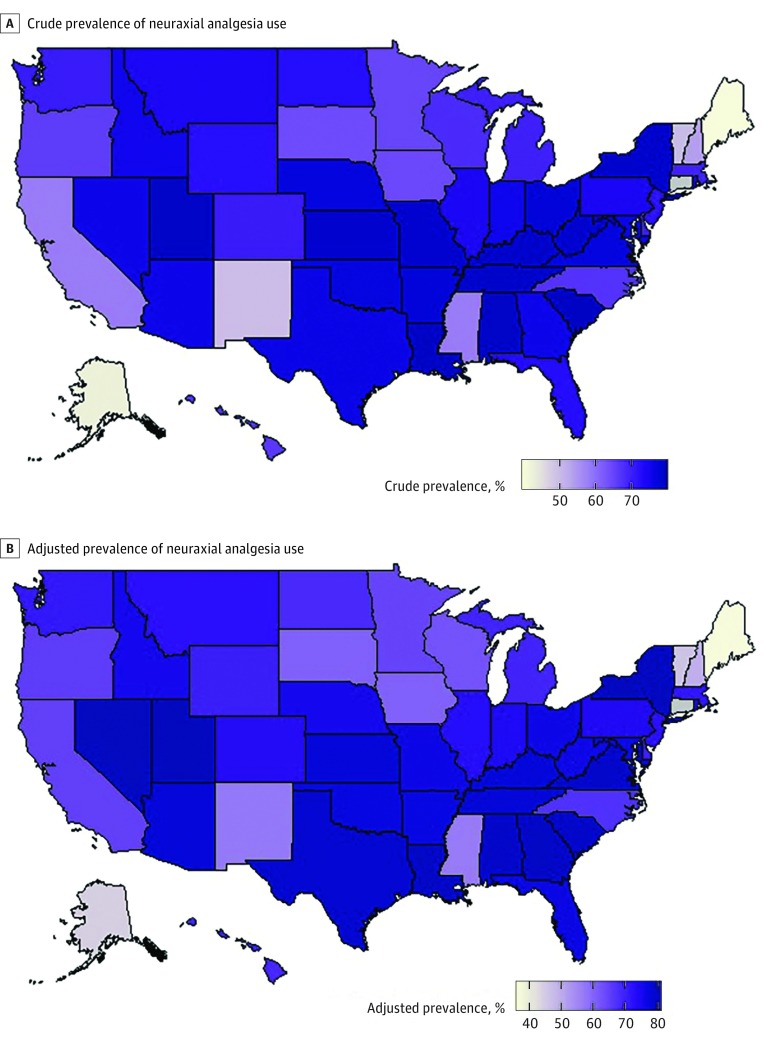
Results: In the study population of 2 625 950 women, 0.1% (n = 2010) were younger than 15 years, 7.0% (n = 183 546) were between the ages of 15 and 19 years, 23.6% (n = 620 118) were between the ages of 20 and 24 years, 29.6% (n = 777 957) were between the ages of 25 and 29 years, 26.0% (n = 683 656) were between the ages of 30 and 34 years, 11.4% (n = 298 237) were between the ages of 35 and 39 years, 2.2% (n = 57 130) were between the ages of 40 and 44 years, and 0.1% (n = 3296) were between the ages of 45 and 54 years. More than 90% were privately insured or insured with Medicaid. Neuraxial analgesia was used by 73.1% (n = 1 920 368) of women. After adjustment for antepartum, obstetric, and intrapartum factors, Maine had the lowest neuraxial analgesia prevalence (36.6%; 95% CI, 33.2%-40.1%) and Nevada the highest (80.1%; 95% CI, 78.3%-81.7%). The adjusted median odds ratio was 1.5 (95% CI, 1.4-1.6), and the intraclass correlation coefficient was 5.4% (95% CI, 4.0%-7.9%).
Conclusions and relevance: Results of this study suggest that a small portion of the overall variation in neuraxial analgesia use is explained by US states. Unmeasured patient-level and hospital-level factors likely account for a large portion of the variation between states. Efforts should be made to understand what the main reasons are for this variation and whether the variation influences maternal or perinatal outcomes.
Conflict of interest statement
Figures