

Association of Changes in Creatinine and Potassium Levels After Initiation of Renin Angiotensin Aldosterone System Inhibitors With Emergency Department Visits, Hospitalizations, and Mortality in Individuals With Chronic Kidney Disease
- PMID: 30646338
- PMCID: PMC6324397
- DOI: 10.1001/jamanetworkopen.2018.3874
Association of Changes in Creatinine and Potassium Levels After Initiation of Renin Angiotensin Aldosterone System Inhibitors With Emergency Department Visits, Hospitalizations, and Mortality in Individuals With Chronic Kidney Disease
Abstract
Importance: Renin angiotensin aldosterone system inhibitors (RAASIs) benefit individuals with chronic kidney disease (CKD). Elevations in serum creatinine and potassium levels are common reasons for discontinuation of this therapy, but their incidence and risks are not well characterized in community practice.
Objective: To evaluate associations of increased creatinine levels, hyperkalemia, and therapy continuation with the risk of emergency department (ED) visits, hospitalizations, and mortality within 1 year after RAASI therapy initiation in individuals with CKD.
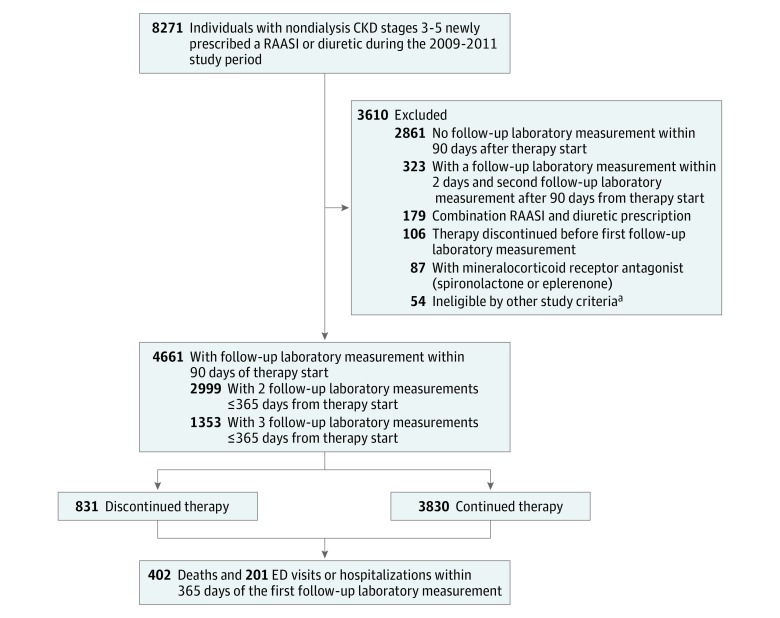
Design, setting, and participants: This prospective cohort study included 4661 individuals with nondialysis CKD newly prescribed a RAASI or a diuretic who were treated at 36 outpatient primary care offices affiliated with Brigham & Women's Hospital and Massachusetts General Hospital, Boston, from January 1, 2009, through December 31, 2011. Individuals receiving a new prescription for a diuretic were used to provide context. All participants had a baseline measure of renal function and at least 1 follow-up measurement of creatinine and potassium levels within 90 days of the prescription. Data were analyzed from January 1, 2009, through December 31, 2012.
Exposures: Changes in creatinine and potassium levels within 90 days after the prescription date and therapy discontinuation.
Main outcomes and measures: Emergency department visits, hospitalizations, and mortality within 1 year.
Results: A total of 4661 individuals were included in the analysis (2506 [53.8%] women; mean [SD] age, 71 [14]; 3931 [84.3%] white; and 4198 [90.1%] with CKD stage 3). Of these, 2354 individuals (50.5%) received RAASIs and 2307 (49.5%) received diuretics. Creatinine level increase of at least 30% after RAASI therapy initiation was found in 158 of 2354 individuals (6.7%); hyperkalemia of greater than 5.0 mEq/L, in 251 of 2354 (10.7%). Increases in creatinine level of at least 30% (unadjusted odds ratio [OR], 1.40; 95% CI, 0.89-2.21), hyperkalemia (unadjusted OR, 1.15; 95% CI, 0.64-2.06), and therapy discontinuation (unadjusted OR, 1.01; 95% CI, 0.71-1.46) were not associated with ED visits or hospitalizations, which was consistent with results from competing risk analyses. Initial increases in creatinine level of at least 30% were associated with mortality in the total cohort (adjusted OR [aOR], 2.17; 95% CI, 1.45-3.25). However, the effect was only independent for diuretics (aOR, 2.27; 95% CI, 1.41-3.66) and not for RAASIs (aOR, 1.82; 95% CI, 0.83-3.99).
Conclusions and relevance: Acute creatinine and potassium level disturbances after initiation of RAASI therapy in individuals with CKD appear to be sustained often often not sustained and not associated with ED visits or hospitalizations, despite therapy continuation. Findings from this study suggest that increases in creatinine level were independently associated with mortality among individuals prescribed diuretics but not RAASIs. Structured laboratory monitoring during RAASI therapy initiation may guide appropriate continuation of therapy in the outpatient setting.
Conflict of interest statement
Figures
Similar articles
-
Lab monitoring and acute care utilization during initiation of renin angiotensin aldosterone inhibitors or diuretics in chronic kidney disease.Medicine (Baltimore). 2019 Dec;98(49):e17963. doi: 10.1097/MD.0000000000017963. Medicine (Baltimore). 2019. PMID: 31804307 Free PMC article.
-
Serum potassium abnormalities, renin-angiotensin-aldosterone system inhibitor discontinuation, and clinical outcomes in patients with chronic cardiovascular, metabolic, and renal conditions: A population-based analysis.Eur J Intern Med. 2024 Jul;125:89-97. doi: 10.1016/j.ejim.2024.03.021. Epub 2024 Mar 27. Eur J Intern Med. 2024. PMID: 38548513
-
Hyperkalemia and renin-angiotensin aldosterone system inhibitor therapy in chronic kidney disease: A general practice-based, observational study.PLoS One. 2019 Mar 7;14(3):e0213192. doi: 10.1371/journal.pone.0213192. eCollection 2019. PLoS One. 2019. PMID: 30845156 Free PMC article.
-
Management of Hyperkalemia in Renin-Angiotensin-Aldosterone System Inhibitor: Strategies to Maintain Chronic Kidney Disease Patients with Type II Diabetes on Therapy.Cardiorenal Med. 2024;14(1):191-201. doi: 10.1159/000538389. Epub 2024 Mar 21. Cardiorenal Med. 2024. PMID: 38513618 Review.
-
Optimally managing hyperkalemia in patients with cardiorenal syndrome.Nephrol Dial Transplant. 2019 Dec 1;34(Suppl 3):iii36-iii44. doi: 10.1093/ndt/gfz225. Nephrol Dial Transplant. 2019. PMID: 31800079 Review.
Cited by
-
Household air pollution as a determinant of health status: A study on older adults in Siliguri Municipal Corporation, India.Sci Rep. 2025 Mar 24;15(1):10048. doi: 10.1038/s41598-025-93311-y. Sci Rep. 2025. PMID: 40122930 Free PMC article.
-
Efficacy and safety of sodium zirconium cyclosilicate for hyperkalaemia: the randomized, placebo-controlled HARMONIZE-Global study.ESC Heart Fail. 2020 Feb;7(1):54-64. doi: 10.1002/ehf2.12561. Epub 2020 Jan 15. ESC Heart Fail. 2020. PMID: 31944628 Free PMC article. Clinical Trial.
-
Long-term safety and efficacy of sodium zirconium cyclosilicate for hyperkalaemia in patients with mild/moderate versus severe/end-stage chronic kidney disease: comparative results from an open-label, Phase 3 study.Nephrol Dial Transplant. 2021 Jan 1;36(1):137-150. doi: 10.1093/ndt/gfz285. Nephrol Dial Transplant. 2021. PMID: 32030422 Free PMC article. Clinical Trial.
-
Sacubitril-valsartan improves conduit vessel function and functional capacity and reduces inflammation in heart failure with reduced ejection fraction.J Appl Physiol (1985). 2021 Jan 1;130(1):256-268. doi: 10.1152/japplphysiol.00454.2020. Epub 2020 Nov 19. J Appl Physiol (1985). 2021. PMID: 33211601 Free PMC article.
-
Managing Hyperkalemia in the Modern Era: A Case-Based Approach.Kidney Int Rep. 2023 Apr 24;8(7):1290-1300. doi: 10.1016/j.ekir.2023.04.016. eCollection 2023 Jul. Kidney Int Rep. 2023. PMID: 37441466 Free PMC article. Review.
References
-
- Maschio G, Alberti D, Janin G, et al. ; The Angiotensin-Converting-Enzyme Inhibition in Progressive Renal Insufficiency Study Group . Effect of the angiotensin-converting-enzyme inhibitor benazepril on the progression of chronic renal insufficiency. N Engl J Med. 1996;334(15):-. doi:10.1056/NEJM199604113341502 - DOI - PubMed
-
- Bakris GL, Sarafidis PA, Weir MR, et al. ; ACCOMPLISH Trial investigators . Renal outcomes with different fixed-dose combination therapies in patients with hypertension at high risk for cardiovascular events (ACCOMPLISH): a prespecified secondary analysis of a randomised controlled trial. Lancet. 2010;375(9721):1173-1181. doi:10.1016/S0140-6736(09)62100-0 - DOI - PubMed
-
- Agodoa LY, Appel L, Bakris GL, et al. ; African American Study of Kidney Disease and Hypertension (AASK) Study Group . Effect of ramipril vs amlodipine on renal outcomes in hypertensive nephrosclerosis: a randomized controlled trial. JAMA. 2001;285(21):2719-2728. doi:10.1001/jama.285.21.2719 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
