

Racial Disparities in Patient Characteristics and Survival After Acute Myocardial Infarction
- PMID: 30646346
- PMCID: PMC6324589
- DOI: 10.1001/jamanetworkopen.2018.4240
Racial Disparities in Patient Characteristics and Survival After Acute Myocardial Infarction
Abstract
Importance: Black patients experience worse outcomes than white patients following acute myocardial infarction (AMI).
Objective: To examine the degree to which nonrace characteristics explain observed survival differences between white patients and black patients following AMI.
Design, setting, and participants: This cohort study used the extensive socioeconomic and clinical characteristics from patients recovering from an AMI that were prospectively collected at 31 hospitals across the contiguous United States between 2003 and 2008 for the Prospective Registry Evaluating Myocardial Infarction: Events and Recovery registry and the Translational Research Investigating Underlying Disparities in Acute Myocardial Infarction Patients' Health Status registry. Survival was assessed using data from the National Death Index. Data were analyzed from December 2016 to July 2018.
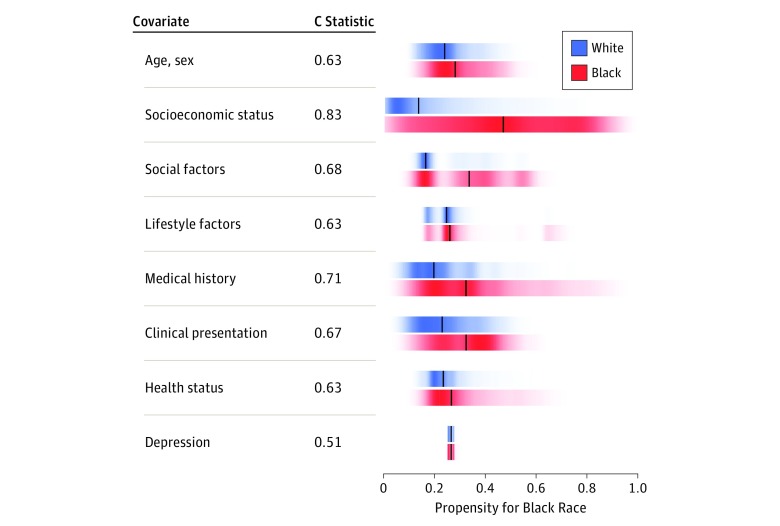
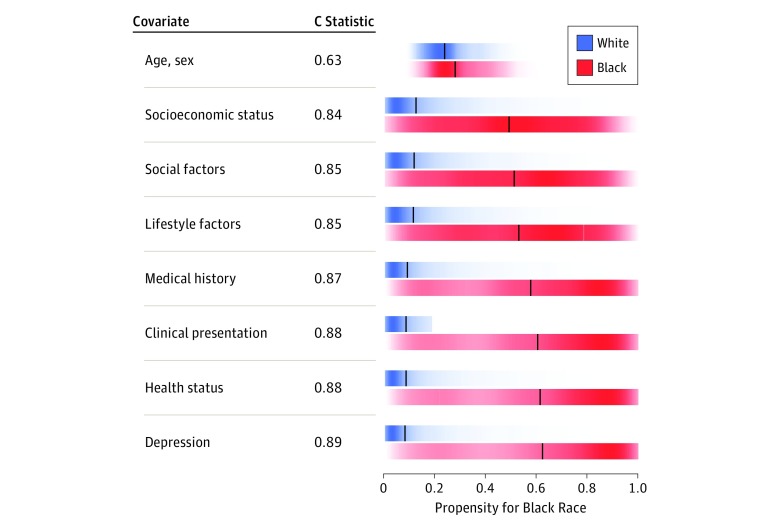
Main outcomes and measures: Patient characteristics were categorized into 8 domains, and the degree to which each domain discriminated self-identified black patients from white patients was determined by calculating propensity scores associated with black race for each domain as well as cumulatively across all domains. The final propensity score was associated with 1- and 5-year mortality rates.
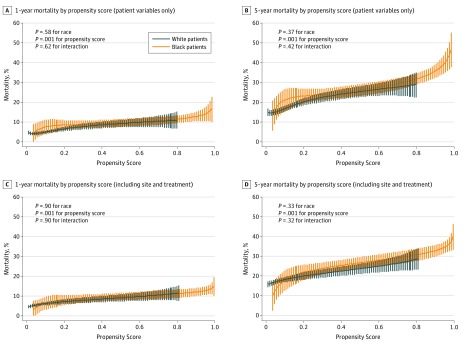
Results: Among 6402 patients (mean [SD] age, 60 [13] years; 2127 [33.2%] female; 1648 [25.7%] black individuals), the 5-year mortality rate following AMI was 28.9% (476 of 1648) for black patients and 18.0% (856 of 4754) for white patients (hazard ratio, 1.72; 95% CI, 1.54-1.92; P < .001). Most categories of patient characteristics differed substantially between black patients and white patients. The cumulative propensity score discriminated race, with a C statistic of 0.89, and the propensity scores were associated with 1- and 5-year mortality rates (hazard ratio for the 75th percentile of the propensity score vs 25th percentile, 1.72; 95% CI, 1.43-2.08; P < .001). Patients in the lowest propensity score quintile associated with being a black individual (regardless of whether they were of white or black race) had a 5-year mortality rate of 15.5%, while those in the highest quintile had a 5-year mortality rate of 31.0% (P < .001). After adjusting for the propensity associated with being a black patient, there was no significant mortality rate difference by race (adjusted hazard ratio, 1.09; 95% CI, 0.93-1.26; P = .37) and no statistical interaction between race and propensity score (P = .42).
Conclusions and relevance: Characteristics of black patients and white patients differed significantly at the time of admission for AMI. Those characteristics were associated with an approximately 3-fold difference in 5-year mortality rate following AMI and mediated most of the observed mortality rate difference between the races.
Conflict of interest statement
Figures
Similar articles
-
Association of Racial and Socioeconomic Disparities With Outcomes Among Patients Hospitalized With Acute Myocardial Infarction, Heart Failure, and Pneumonia: An Analysis of Within- and Between-Hospital Variation.JAMA Netw Open. 2018 Sep 7;1(5):e182044. doi: 10.1001/jamanetworkopen.2018.2044. JAMA Netw Open. 2018. PMID: 30646146 Free PMC article.
-
Cardiovascular Disease Events and Mortality After Myocardial Infarction Among Black and White Adults: REGARDS Study.Circ Cardiovasc Qual Outcomes. 2020 Dec;13(12):e006683. doi: 10.1161/CIRCOUTCOMES.120.006683. Epub 2020 Dec 11. Circ Cardiovasc Qual Outcomes. 2020. PMID: 33302710 Free PMC article.
-
Impact of Race on the In-Hospital Quality of Care Among Young Adults With Acute Myocardial Infarction.J Am Heart Assoc. 2021 Sep 7;10(17):e021408. doi: 10.1161/JAHA.121.021408. Epub 2021 Aug 25. J Am Heart Assoc. 2021. PMID: 34431311 Free PMC article.
-
Ethnic and Racial Disparities in Acute Myocardial Infarction.Curr Cardiol Rep. 2020 Jul 9;22(9):88. doi: 10.1007/s11886-020-01351-9. Curr Cardiol Rep. 2020. PMID: 32648143 Review.
-
Racial Disparity Between the Post-Procedural Outcomes Among Patients With Peripheral Artery Disease: A Systematic Review and Meta-analysis.Curr Probl Cardiol. 2023 May;48(5):101595. doi: 10.1016/j.cpcardiol.2023.101595. Epub 2023 Jan 21. Curr Probl Cardiol. 2023. PMID: 36690312
Cited by
-
Smoking cessation behavior in patients with a diagnosis of a non-communicable disease: The impact of perceived disease severity of and susceptibility to the disease.Tob Induc Dis. 2023 Oct 6;21:125. doi: 10.18332/tid/170430. eCollection 2023. Tob Induc Dis. 2023. PMID: 37808588 Free PMC article.
-
Outcomes of ST-elevation myocardial infarction by age and sex in a low-income urban community: The Montefiore STEMI Registry.Clin Cardiol. 2020 Oct;43(10):1100-1109. doi: 10.1002/clc.23412. Epub 2020 Jul 28. Clin Cardiol. 2020. PMID: 33460205 Free PMC article.
-
Presentation, management, and early outcomes of young acute coronary syndrome patients- analysis of 23,560 South Asian patients from 2012 to 2021.BMC Cardiovasc Disord. 2024 Jul 19;24(1):378. doi: 10.1186/s12872-024-04036-1. BMC Cardiovasc Disord. 2024. PMID: 39030502 Free PMC article.
-
Trends in Premature Mortality From Acute Myocardial Infarction in the United States, 1999 to 2019.J Am Heart Assoc. 2022 Jan 4;11(1):e021682. doi: 10.1161/JAHA.121.021682. Epub 2021 Dec 22. J Am Heart Assoc. 2022. PMID: 34935456 Free PMC article.
-
Association of insurance status with potentially avoidable transfers to an academic emergency department: A retrospective observational study.J Am Coll Emerg Physicians Open. 2021 Mar 6;2(2):e12385. doi: 10.1002/emp2.12385. eCollection 2021 Apr. J Am Coll Emerg Physicians Open. 2021. PMID: 33733247 Free PMC article.
References
-
- Dehmer GJ, Weaver D, Roe MT, et al. . A contemporary view of diagnostic cardiac catheterization and percutaneous coronary intervention in the United States: a report from the CathPCI Registry of the National Cardiovascular Data Registry, 2010 through June 2011. J Am Coll Cardiol. 2012;60(20):-. doi:10.1016/j.jacc.2012.08.966 - DOI - PubMed
