

Motivators, Barriers, and Facilitators to Traveling to the Safest Hospitals in the United States for Complex Cancer Surgery
- PMID: 30646367
- PMCID: PMC6324377
- DOI: 10.1001/jamanetworkopen.2018.4595
Motivators, Barriers, and Facilitators to Traveling to the Safest Hospitals in the United States for Complex Cancer Surgery
Abstract
Importance: Directing patients to safer hospitals for complex cancer surgery (regionalization) may prevent thousands of mortalities in the United States.
Objective: To understand the potential for individuals to move to safer hospitals: what would inspire them to travel (motivators), what challenges would they face (barriers), and what would enable them to travel (facilitators).
Design, setting, and participants: This nationally representative online survey study asked respondents to consider complex cancer surgery at their local hospital or a hospital specializing in cancer an hour farther away. Completed surveys were weighted across sociodemographics to be nationally representative and outcomes were reported as weighted percentages. In January 2018, a panel of 1817 US adults recruited by address- and telephone-based sampling to be nationally representative were invited to take the survey. Data analysis was conducted from January 24, 2018, to September 19, 2018.
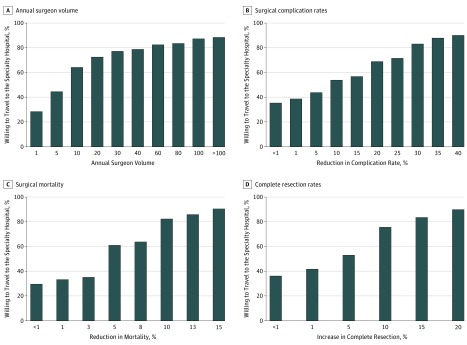
Main outcomes and measures: Proportion of respondents motivated to travel by specific quality and safety indicators (motivators), magnitude in difference that would be necessary, proportion facing specific barriers, and proportion enabled to move by facilitators. Resistant individuals were identified as people who would not travel except for the largest (top quartile) outcomes differences.
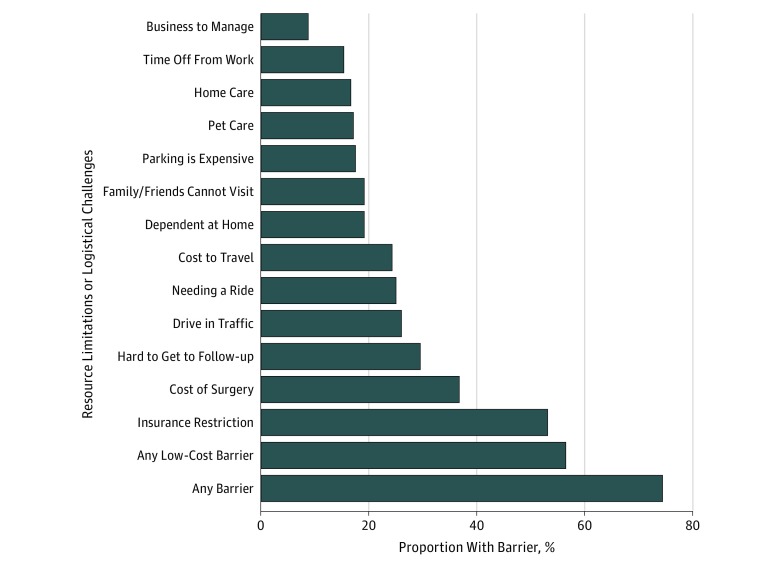
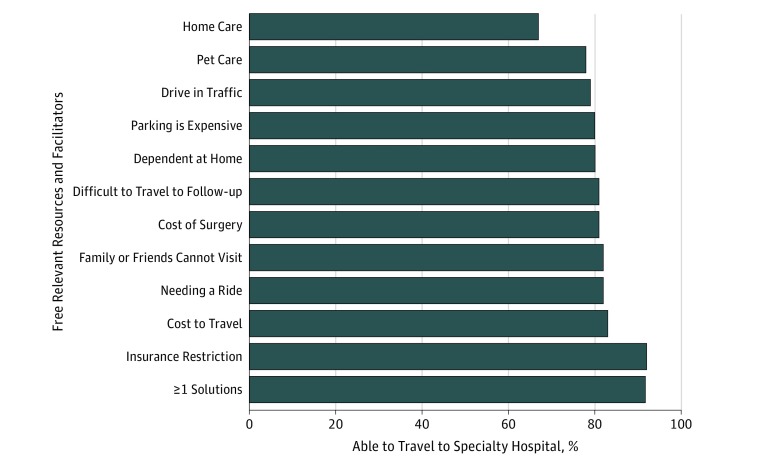
Results: There were 1016 completed surveys (response rate of 55.9%). The weighted median age was 48 years, 52% were female, median annual income was between $60 000 and $75 000, and 85% lived in a metropolitan area. Nonresponders were more likely than responders to be female, younger, nonwhite, less educated, and lower income (female: 54.4% vs 48.3%; P = .01; younger [aged <45 years]: 56.3% vs 37.1%; P < .001; nonwhite: 41.6% vs 30.0%; P < .001; less than college education: 43.8% vs 32.4%; P < .001; income <$30 000: 22.1% vs 17.1%; P = .01). Superior safety or oncologic outcomes, presented separately, motivated an average of 92% of respondents (95% CI, 90%-94%) to travel. One-third were easily motivated, requiring less than 1% advantage in safety or quality, while 12% were particularly resistant across outcomes. Respondents with lower income (income <$25 000: odds ratio, 2.01; 95% CI, 1.19-3.39) and nonwhite race (odds ratio, 1.60; 95% CI, 1.05-2.42) were more resistant to travel. At least 1 barrier was identified by 74% of respondents (95% CI, 72%-77%), most commonly financial (costs/insurance). However, 94% of respondents (95% CI, 92%-96%) with barriers would travel if provided facilitators, many of which were relatively low cost (transportation, parking, and hotel).
Conclusions and relevance: It appears that most of the US public could be motivated to travel to safer hospitals for complex cancer surgery, yet most would require some support to move. Further efforts to ensure that benefits from regionalization are equitable across sociodemographic strata are indicated.
Conflict of interest statement
Figures
Comment in
-
Regionalization of Complex Cancer Surgery: How, When, and Why?JAMA Netw Open. 2018 Nov 2;1(7):e184586. doi: 10.1001/jamanetworkopen.2018.4586. JAMA Netw Open. 2018. PMID: 30646363 No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
