

Changes in the US Burden of Chronic Kidney Disease From 2002 to 2016: An Analysis of the Global Burden of Disease Study
- PMID: 30646390
- PMCID: PMC6324659
- DOI: 10.1001/jamanetworkopen.2018.4412
Changes in the US Burden of Chronic Kidney Disease From 2002 to 2016: An Analysis of the Global Burden of Disease Study
Abstract
Introduction: Over the past 15 years, changes in demographic, social, and epidemiologic trends occurred in the United States. These changes likely contributed to changes in chronic kidney disease (CKD) epidemiology.
Objective: To describe the change in burden of CKD at the US state level from 2002 to 2016.
Design, setting, and participants: This systematic analysis used data and methodologies from the 2016 Global Burden of Disease study in the United States. Data on CKD from 2002 to 2016 were examined at the state level.
Main outcomes and measures: Disability-adjusted life years (DALYs) and death due to CKD.
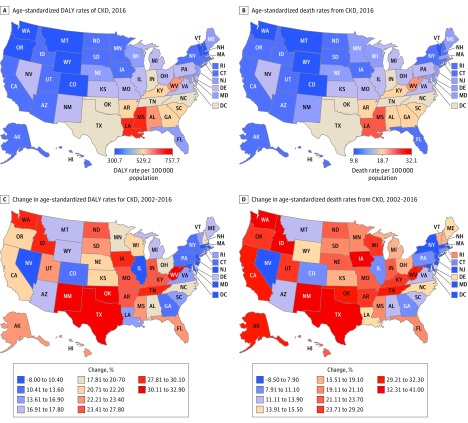
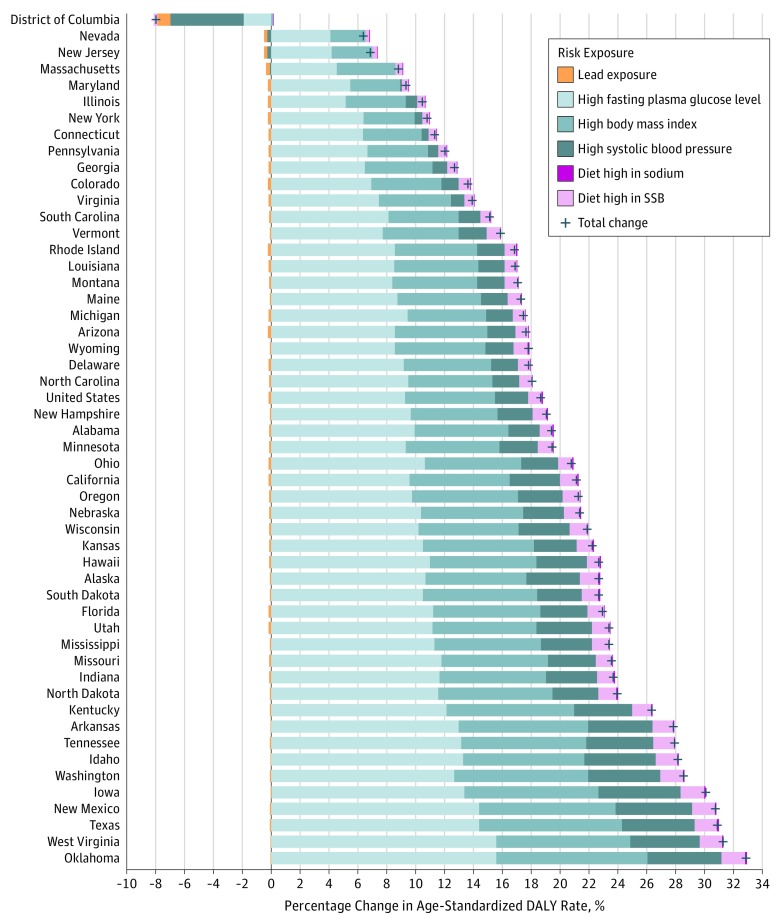
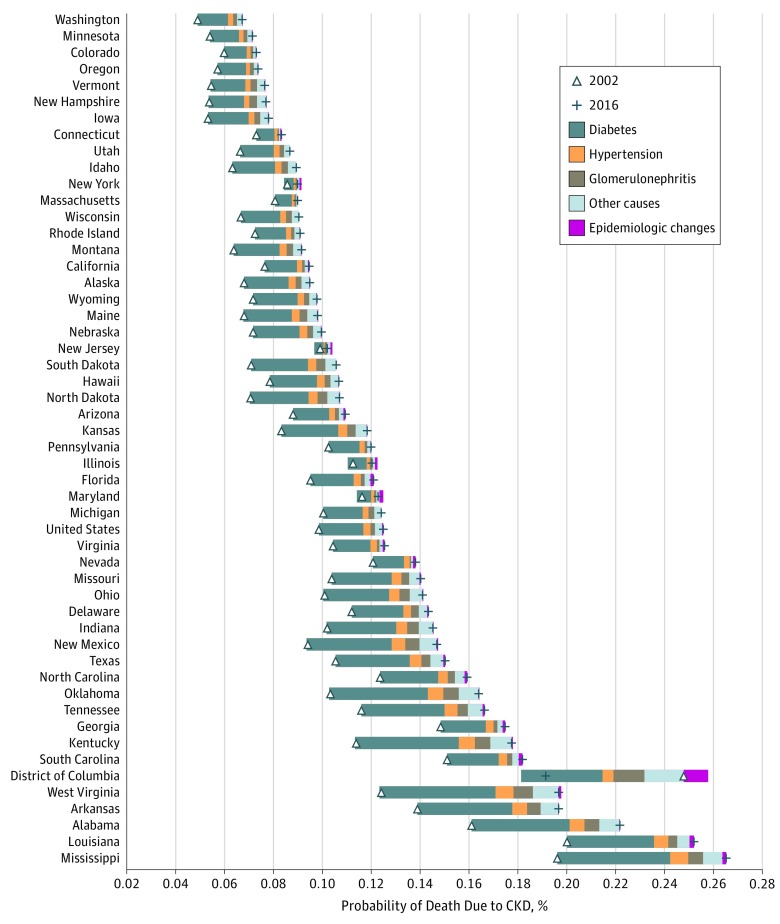
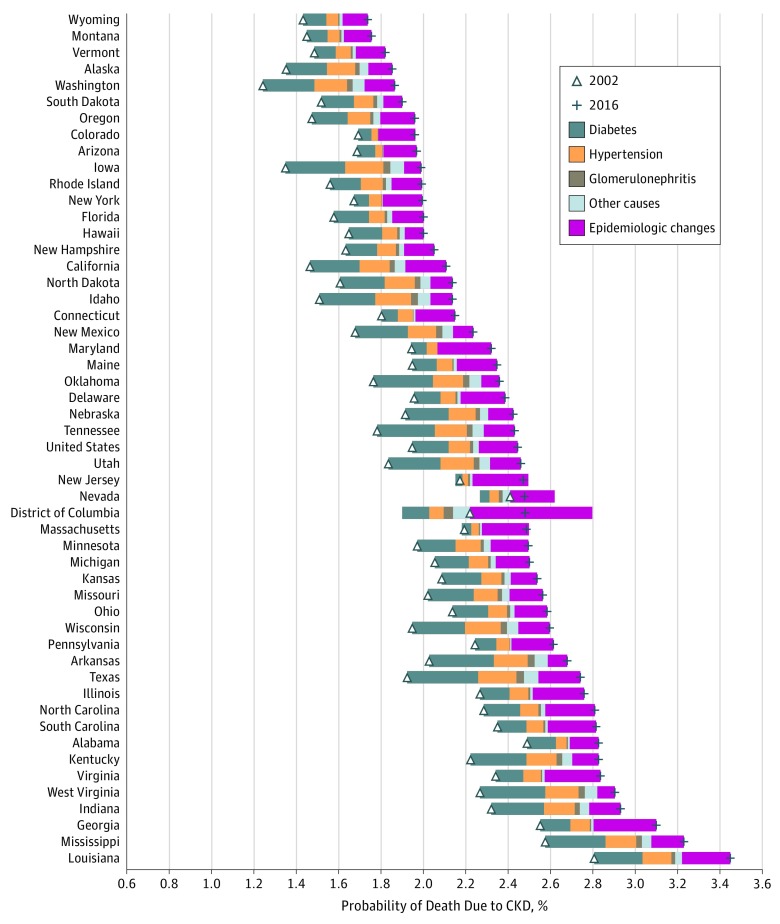
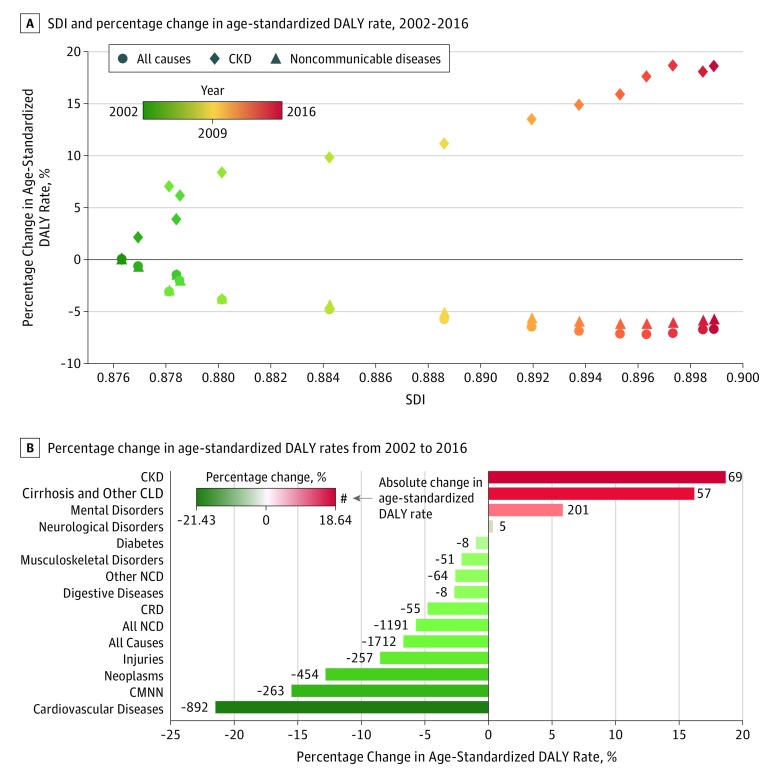
Results: In this analysis of data from individuals in the United States, from 2002 to 2016, CKD DALYs increased by 52.6%, from 1 269 049 DALYs (95% uncertainty interval [UI], 1 154 521-1 387 008) to 1 935 954 DALYs (95% UI, 1 747 356-2 124 795). Death due to CKD increased by 58.3%, from 52 127 deaths (95% UI, 51 082-53 076) to 82 539 deaths (95% UI, 80 298-84 652). All states exhibited increases in CKD burden, but the rate of change (2002-2016) and the burden in 2016 varied by state. States in the southern United States (including Mississippi and Louisiana) exhibited more than twice the burden seen in other states (eg, the age-standardized CKD DALY rate in Vermont was 321 [95% UI, 281-363] per 100 000 population, whereas the rate in Mississippi was 697 [95% UI, 620-779] per 100 000 population). In the United States, the increase in CKD DALYs was attributable to increased risk exposure (40.3%), aging (32.3%), and population growth (27.4%). Age-standardized CKD DALY rates increased by 18.6% where increases in metabolic, and to a lesser extent dietary, risk factors contributed 93.8% and 5.3% of this change, respectively. Chronic kidney disease due to diabetes was the primary contributor for the 26.8% increased probability of death due to CKD among the population aged 20 to 54 years; among the population aged 55 to 89 years, the probability of death due to CKD increased by 25.6% and was driven by CKD due to diabetes and decreased probability of death from causes other than CKD. Improvement in sociodemographic development was coupled with an increase in age-standardized CKD DALY rates that occurred at a faster pace than that of other noncommunicable diseases in the United States.
Conclusions and relevance: Our findings revealed that between 2002 and 2016, the burden of CKD in the United States appeared to be increasing and variable among states. These changes may be associated with increased risk exposure and demographic expansion leading to increased probability of death due to CKD, especially among young adults. The findings suggest that an effort to target the reduction of CKD through greater attention to metabolic and dietary risks, especially among younger adults, is necessary.
Conflict of interest statement
Figures
References
-
- Nathan Keyfitz WF. World Population Growth and Aging: Demographic Trends in the Late Twentieth Century. Chicago, IL: University of Chicago Press; 1990.
-
- Our World in Data Our World in Data website. https://ourworldindata.org/. Accessed January 15, 2018.
-
- GBD 2016 Risk Factors Collaborators Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1345-1422. doi:10.1016/S0140-6736(17)32366-8 - DOI - PMC - PubMed
-
- GBD 2015 Healthcare Access and Quality Collaborators Healthcare Access and Quality Index based on mortality from causes amenable to personal health care in 195 countries and territories, 1990-2015: a novel analysis from the Global Burden of Disease Study 2015. Lancet. 2017;390(10091):231-266. doi:10.1016/S0140-6736(17)30818-8 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
