

A US National Study of the Association Between Income and Ambulance Response Time in Cardiac Arrest
- PMID: 30646394
- PMCID: PMC6324393
- DOI: 10.1001/jamanetworkopen.2018.5202
A US National Study of the Association Between Income and Ambulance Response Time in Cardiac Arrest
Abstract
Importance: Emergency medical services (EMS) provide critical prehospital care, and disparities in response times to time-sensitive conditions, such as cardiac arrest, may contribute to disparities in patient outcomes.
Objectives: To investigate whether ambulance 9-1-1 times were longer in low-income vs high-income areas and to compare response times with national benchmarks of 4, 8, or 15 minutes across income quartiles.
Design, setting, and participants: A retrospective cross-sectional study was performed of the 2014 National Emergency Medical Services Information System data in June 2017 using negative binomial and logistic regressions to examine the association between zip code-level income and EMS response times. The study used ambulance 9-1-1 response data for out-of-hospital cardiac arrest from 46 of 50 state repositories (92.0%) in the United States. The sample included 63 600 cardiac arrest encounters of patients who did not die on scene and were transported to the hospital.
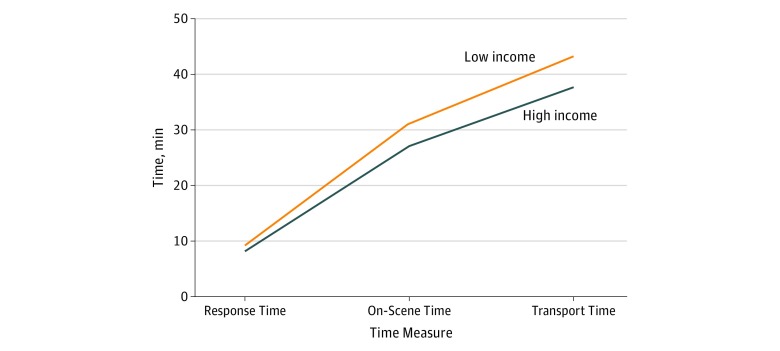
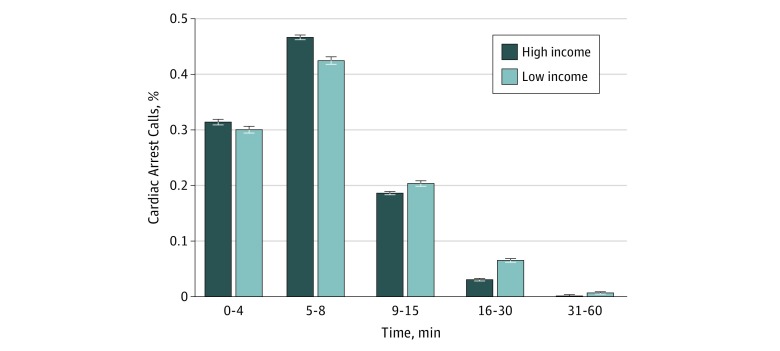
Main outcomes and measures: Four time measures were examined, including response time, on-scene time, transport time, and total EMS time. The study compared response times with EMS response time benchmarks for responding to cardiac arrest calls within 4, 8, and 15 minutes.
Results: The study sample included 63 600 cardiac arrest encounters of patients (mean [SD] age, 60.6 [19.0] years; 57.9% male), with 37 550 patients (59.0%) from high-income areas and 8192 patients (12.9%) from low-income areas. High-income areas had greater proportions of white patients (70.1% vs 62.2%), male patients (58.8% vs 54.1%), privately insured patients (29.4% vs 15.9%), and uninsured patients (15.3% vs 7.9%), while low-income areas had a greater proportion of Medicaid-insured patients (38.3% vs 15.8%). The mean (SD) total EMS time was 37.5 (13.6) minutes in the highest zip code income quartile and 43.0 (18.8) minutes in the lowest. After controlling for urban zip code, weekday, and time of day in regression analyses, total EMS time remained 10% longer (95% CI, 9%-11%; P < .001), translating to 3.8 minutes longer in the poorest zip codes. The EMS response time to patients in high-income zip codes was more likely to meet 8-minute and 15-minute cutoffs compared with low-income zip codes.
Conclusions and relevance: Patients with cardiac arrest from the poorest neighborhoods had longer EMS times compared with those from the wealthiest, and response times were less likely to meet national benchmarks in low-income areas, which may lead to increased disparities in prehospital delivery of care over time.
Conflict of interest statement
Figures
Comment in
-
Income and Ambulance Response Time Inequality: No Simple Explanation, No Simple Fix.JAMA Netw Open. 2018 Nov 2;1(7):e185201. doi: 10.1001/jamanetworkopen.2018.5201. JAMA Netw Open. 2018. PMID: 30646387 No abstract available.
References
-
- Smedley BD, Stith AY, Nelson AR, eds. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Washington, DC: National Academies Press; 2003. - PubMed
-
- Office of Disease Prevention and Health Promotion 2020 Topics and objectives: access to health services. https://www.healthypeople.gov/2020/topics-objectives/topic/Access-to-Hea.... Published 2017. Accessed February 9, 2018.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
