Assessment of Esophageal Motor Disorders Using High-resolution Manometry in Esophageal Dysphagia With Normal Endoscopy
- PMID: 30646476
- PMCID: PMC6326201
- DOI: 10.5056/jnm18042
Assessment of Esophageal Motor Disorders Using High-resolution Manometry in Esophageal Dysphagia With Normal Endoscopy
Abstract
Background/aims: The distribution and esophageal motor characteristics of Chinese patients with esophageal dysphagia who exhibit no structural abnormalities on esophagogastroduodenoscopy remain unclear. Our aim is to assess the esophageal motor patterns using high-resolution manometry (HRM) and classify them according to the Chicago classification version 3.0 (CC v3.0). Furthermore, we compared the CC v3.0 and the previous version 2.0 (CC v2.0) for diagnosis of motor disorders.
Methods: Two hundred thirty-six (mean age 48.4 ± 12.2 years, 61.9% female) patients with esophageal dysphagia were included for analysis of motor function using HRM. All participants were administered a questionnaire to determine Eckardt scores before HRM.
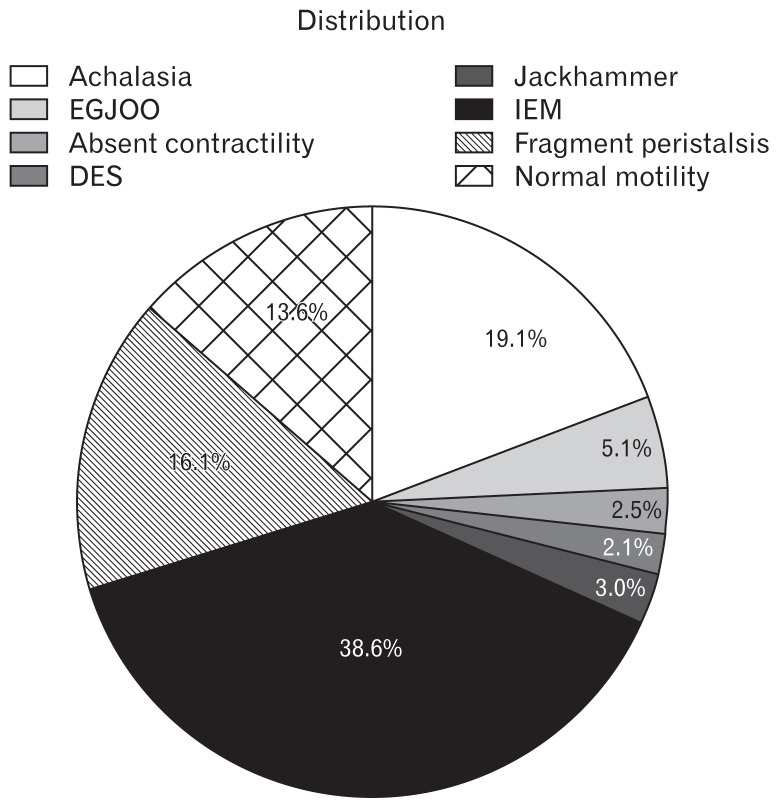
Results: According to the CC v3.0, 57 (24.2%) patients showed evidence of esophagogastric junction outflow obstruction and were classified as Group 1. Eighteen (7.6%) patients with major disorders of peristalsis were classified as Group 2. Minor disorders of peristalsis (Group 3) were much more frequent (129 [54.7%] patients). Thirty-two (13.6%) patients had normal esophageal manometry were classified as Group 4. All patients with abnormal pH or pH impedance monitoring (n = 44) had minor motor disorders (ineffective esophageal motility [IEM] = 34, fragmented peristalsis = 10). Based on motor category, the Eckardt score was 4.7 ± 0.1 in Group 1, 4.5 ± 0.3 in Group 2, 3.5 ± 0.1 in Group 3, and 3.9 ± 0.1 in Group 4.
Conclusions: IEM was the most common esophageal motor disorder in patients with esophageal dysphagia who showed no structural abnormality on endoscopy. While a high Eckardt score suggests outflow obstruction or a major motor disorder, a low score suggests IEM.
Keywords: Dysphagia; Endoscopy, digestive system; Esophageal motility disorder; Manometry.
Conflict of interest statement
Figures


References
LinkOut - more resources
Full Text Sources