Combined Multichannel Intraluminal Impedance and High-resolution Manometry Improves Detection of Clinically Relevant Esophagogastric Junction Outflow Obstruction
- PMID: 30646478
- PMCID: PMC6326198
- DOI: 10.5056/jnm18148
Combined Multichannel Intraluminal Impedance and High-resolution Manometry Improves Detection of Clinically Relevant Esophagogastric Junction Outflow Obstruction
Abstract
Background/aims: Esophagogastric junction outflow obstruction (EGJOO) is a diagnostically heterogeneous group with variable clinical relevance. We studied whether evaluation of bolus transit by multichannel intraluminal impedance (MII) is useful for discriminating clinically relevant EGJOO.
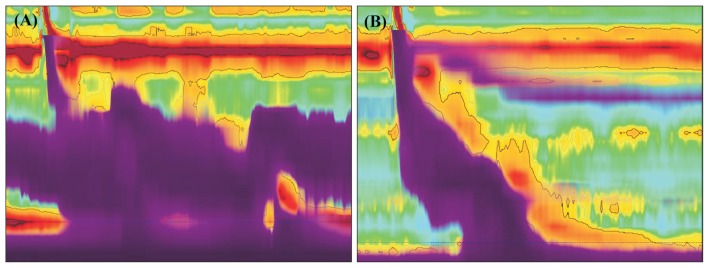
Methods: A total 169 patients diagnosed as having EGJOO between June 2011 and February 2018 were analyzed. All the patients received a combined MII and high-resolution manometry (CMII-HRM). MII was reported as having abnormal liquid bolus transit (LBT) if < 80% of swallows had complete bolus transit. EGJOO was defined as a median integrated relaxation pressure of > 20 mmHg and when the criteria for achalasia were not met. Patients who progress to achalasia, show significant passage disturbance, or require pneumatic dilatation were defined as having a clinically relevant EGJOO.
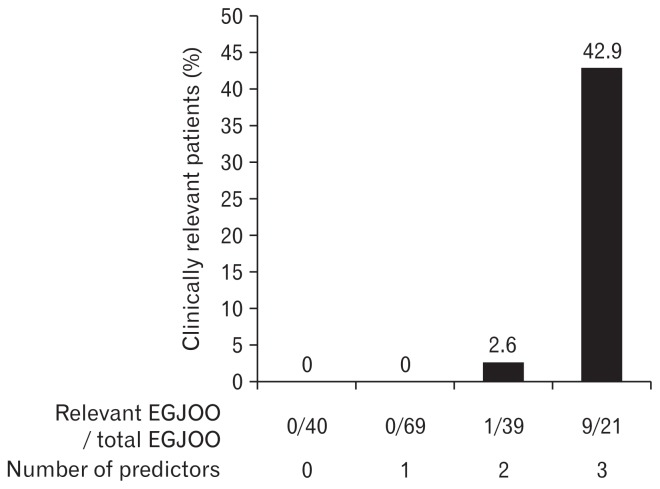
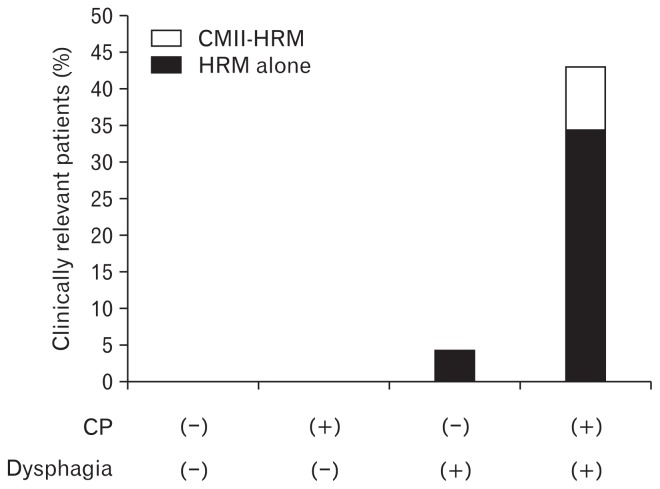
Results: Among the patients with EGJOO (n = 169), the clinically relevant group (n = 10) is more likely to have dysphagia (100% vs 25.2%, P < 0.001), compartmentalized pressurization (CP; 90.0% vs 22.0%, P < 0.001), and abnormal LBT (100% vs 66.7%, P = 0.032) compared to the non-relevant group (n = 159). The combination of dysphagia, CP, and abnormal LBT showed the best predictive power for clinically relevant EGJOO (sensitivity 90%, specificity 92.5%, positive predictive value 42.9%, negative predictive value 99.3%, positive likelihood ratio 11.9, and negative likelihood ratio 0.1). When CMII-HRM was used, an additional 8.3% of clinically relevant EGJOO cases were identified as compared with HRM alone.
Conclusion: Clinically relevant EGJOO can be predicted using CMII-HRM.
Keywords: Electric impedance; Esophageal achalasia; Esophagogastric junction; Manometry.
Conflict of interest statement
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous