

Epidemiology of non-traumatic spinal cord injury in Uganda: a single center, prospective study with MRI evaluation
- PMID: 30646840
- PMCID: PMC6332574
- DOI: 10.1186/s12883-019-1236-3
Epidemiology of non-traumatic spinal cord injury in Uganda: a single center, prospective study with MRI evaluation
Abstract
Background: A few reliable national data concerning the etiology of non-traumatic spinal cord injury (SCI) in sub-Sahara Africa exists, mainly because of the limitations of diagnostic imaging. These are both expensive and mostly unavailable in several resource-limited settings. Only a few studies have employed the magnetic resonance imaging (MRI) in documenting non-traumatic SCI and most of these studies are from South Africa. We sought to describe the clinical presentation, MRI radiological patterns, and one-year survival among subjects with non-traumatic SCI in Uganda.
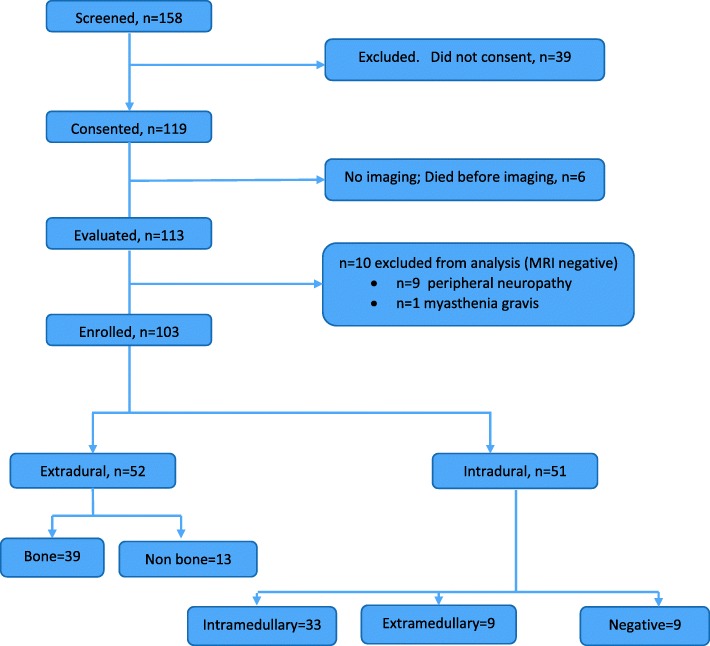
Methods: We enrolled a prospective cohort of 103 participants with non-traumatic SCI at Mulago National Referral Hospital Kampala, Uganda in 2013-2015. Participants received standard of care management, with surgical intervention as needed, with one-year follow up. Data were analyzed using Descriptive statistics.
Results: In 103 participants with non-traumatic SCI, the median (IQR) age was 37 (18, 85) years and 25% of the participants were HIV-infected. Paraplegia/paraparesis was the most common clinical presentation in 70% (n = 72). Severe disease was present in 82% (n = 85) as per American Spinal Injury Association (ASIA) scale A-C. On MRI, 50% had extradural lesions. However, bone lesions accounted for only 75% of all the extradural lesions. More than 60% of the patients had lesions that could only be diagnosed on MRI. Deaths occurred in 42% (n = 44) of participants, with the highest mortality among those with extradural lesions (60%).
Conclusion: The mortality following non-traumatic spinal cord injuries in Uganda is high. We demonstrated an equal distribution between extradural and intradural lesions, which differs from the historical predominance of extradural lesions. Increased utilization of MRI particularly among young age groups is needed to make a diagnosis.
Keywords: MRI; Mortality; Myelopathy; Non-traumatic spinal cord injury; Sub-Saharan Africa; Uganda.
Conflict of interest statement
Ethics approval and consent to participate
Makerere University Research and Ethics Committee and the Uganda National Council for Science and Technology provided ethical approval for the study and all patients provided a written consent to participate in the study.
Consent for publication
This manuscript does not contain any identifiable personal data of the participants and hence the consent for the publication of identifying images or other personal or clinical details of participants that compromise anonymity is not applicable to this manuscript.
Competing interests
David Meya is an Editorial Board Member (associate editor) of BMC Neurology. I declare that there were no competing interests for this work among the other authors.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Brown KG. Non-traumatic paraplegia in sub-Saharan Africa. East Afr Med J. 1979;56(7):300–310. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
