

Factors influencing disability in patients with chronic low back pain attending a tertiary hospital in sub-Saharan Africa
- PMID: 30646894
- PMCID: PMC6334448
- DOI: 10.1186/s12891-019-2403-9
Factors influencing disability in patients with chronic low back pain attending a tertiary hospital in sub-Saharan Africa
Abstract
Background: Very little is known about the burden of chronic low back pain in Africa. This study aimed at assessing disability and associated factors in chronic low back patients in Cameroon.
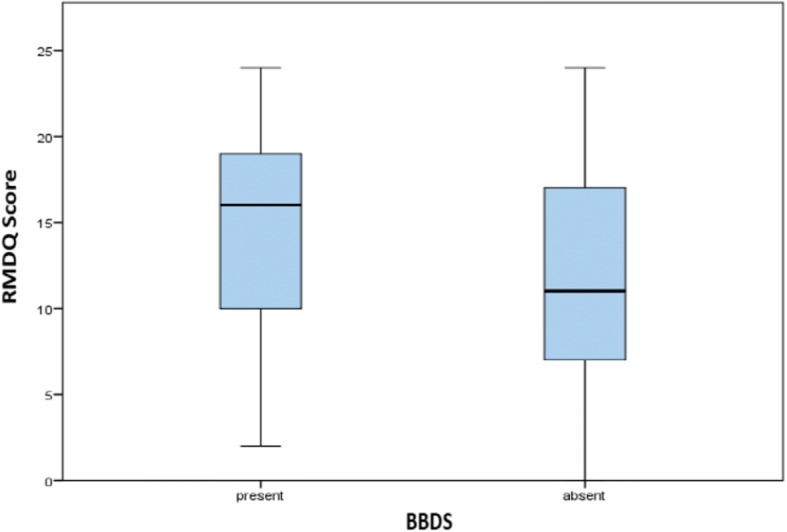
Methods: We carried a hospital-based cross-sectional study including patients suffering from low back pain (LBP) of at least 12 weeks' duration. Disability was assessed using the Roland Morris Disability Questionnaire (RMDQ). RMDQ > 4 described persons with dysfunctional levels of disability. Multivariable linear regression was used to investigate factors associated with higher RMDQ scores hence greater disability. Variables investigated included; gender, age, marital status, employment status and type, smoking history, alcohol consumption, income, pain intensity, LBP duration, psychological wellbeing, sleep satisfaction, leg pain, numbness/paresthesia, bowel/bladder dysfunction symptoms (BBDS), body mass index (BMI), and days of work absence.
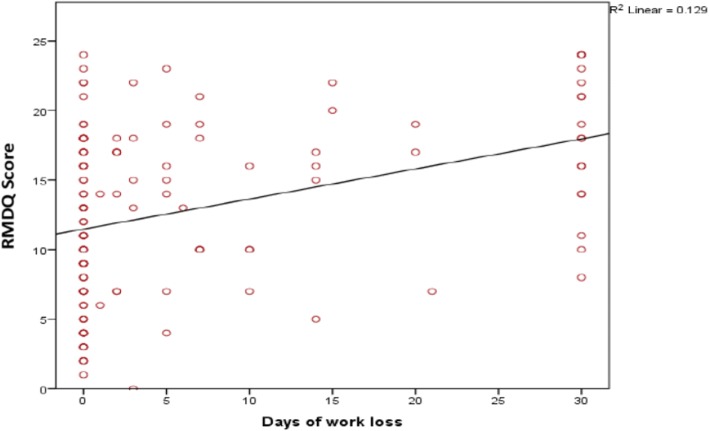
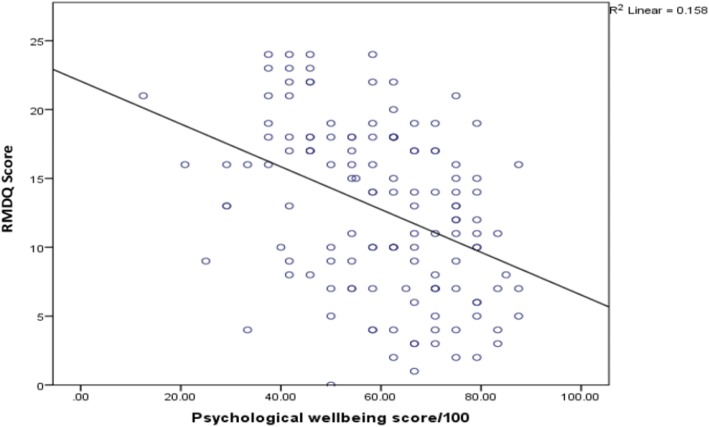
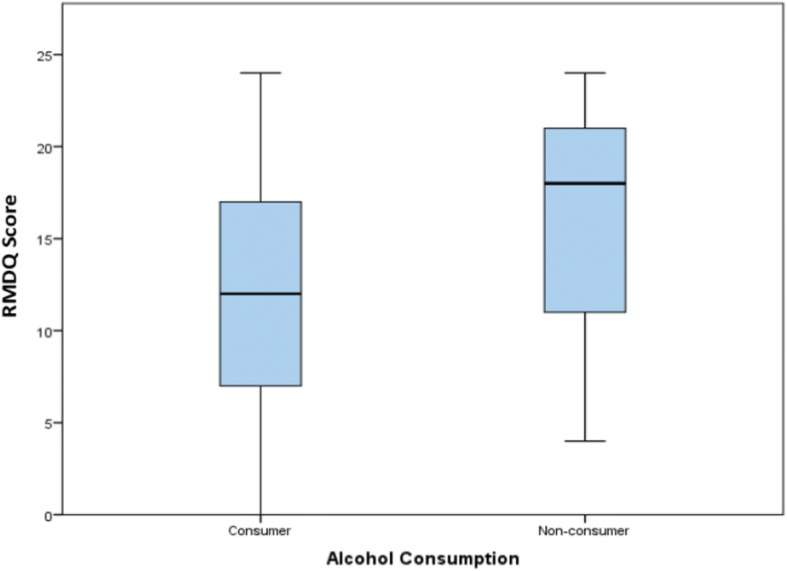
Results: A sample of 136 adults (64% female) with a mean age of 50.6 ± 12.2 years participated in the study. Median duration of LBP was 33 (25th - 75th percentile: 12-81) months. Mean RMDQ score was 12.8 ± 6. In multivariable linear regression, pain intensity (β = 0.07, p = 0.002), longer days of work absence (β = 0.15, p = 0.003) and BBDS (β =2.33, p = 0.029) were associated with greater disability. Factors such as consumption of alcohol (β = - 3.55, p = 0.005) and higher psychological wellbeing scores (β = - 0.10, p = 0.004) significantly contributed to less disability (lower RMDQ scores). Dysfunctional levels of disability were present in 88.1% of patients.
Conclusion: CLBP is associated with significant disability and this relationship is driven by several factors. Multidisciplinary management strategies especially those targeted to improve pain control, manage BBDS and improve psychological wellbeing could reduce disability and improve quality of life.
Keywords: Africa; Chronic low back pain; Disability.
Conflict of interest statement
Authors’ information
Ethics approval and consent to participate
All the patients read and signed an informed consent sheet. Research authorisations were obtained from the administration of Douala General Hospital. Ethical clearance was obtained from the Faculty of Health Sciences Institutional Ethical Review Board of the University of Buea, Cameroon.
Consent for publication
NA
Competing interests
All authors declare no conflict of interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- National Center for Health Statistics (US) Hyattsville (MD): National Center for Health Statistics (US) 2016. Health, United States, 2015: with special feature on racial and ethnic health disparities. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
