

Body mass index as an independent risk factor for inferior vena cava resection during thrombectomy for venous tumor thrombus of renal cell carcinoma
- PMID: 30646899
- PMCID: PMC6334420
- DOI: 10.1186/s12957-019-1560-5
Body mass index as an independent risk factor for inferior vena cava resection during thrombectomy for venous tumor thrombus of renal cell carcinoma
Abstract
Objective: To define preoperative clinical and radiographic risk factors for the need of inferior vena cava (IVC) resection in patients with renal cell carcinoma (RCC) and IVC tumor thrombus.
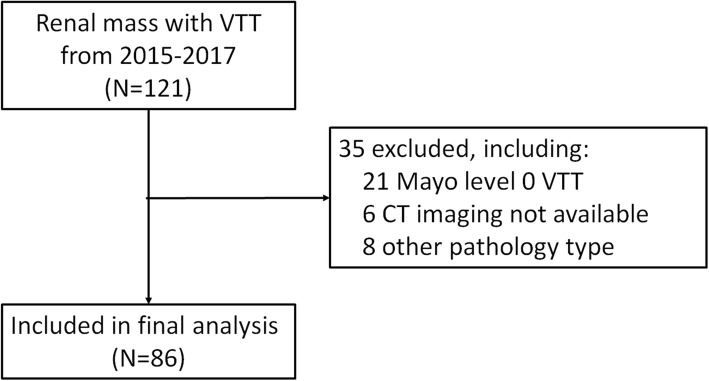
Methods: We reviewed data of 121 patients with renal cell carcinoma and venous tumor thrombus receiving radical nephrectomy and thrombectomy at our institution between 2015 and 2017, and 86 patients with Mayo I-IV level tumor thrombus were included in the final analysis. Clinical features, operation details, and pathology data were collected. Preoperative images were reviewed separately by two radiologists. Univariable and multivariable logistic regression analyses were applied to evaluate clinical and radiographic risk factors of IVC resection.
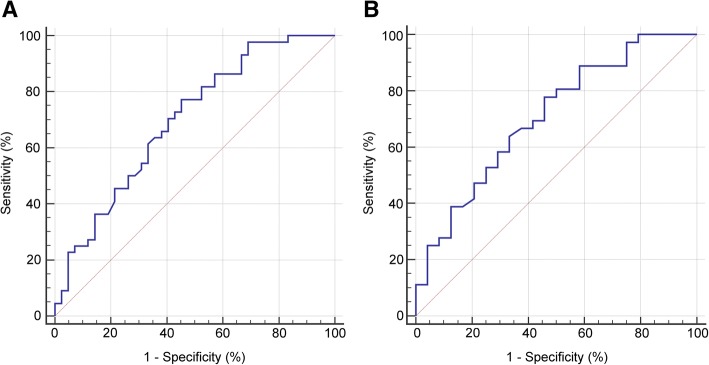
Results: Of the 86 patients, 44 (51.2%) received IVC resection during thrombectomy. In univariate analysis, we found that body mass index (BMI) (odds ratio [OR] = 1.22, P = 0.003), primary tumor diameter (OR = 0.84, P = 0.022), tumor thrombus width (OR = 1.08, P = 0.037), tumor thrombus level (OR = 1.57, P = 0.030), and IVC occlusion (OR = 2.67, P = 0.038) were associated with the need for resection of the IVC. After adjusting for the other factors, BMI (OR = 1.18, P = 0.019) was the only significant risk factor for IVC resection. Multivariable analysis in Mayo II-IV subgroups confirmed BMI as an independent risk factor (OR = 1.26, P = 0.024). A correlation between BMI and the width (Pearson's correlation coefficient [PCC] = 0.27, P = 0.014) and length (PCC = 0.23, P = 0.037) of the tumor thrombus was noticed.
Conclusion: We identified BMI as an independent risk factor for IVC resection during thrombectomy of RCC with tumor thrombus in a Chinese population. More careful preoperative preparation for the IVC resection and/or reconstruction is warranted in patients with higher BMI.
Keywords: Renal cell carcinoma; Risk factor; Thrombectomy; Vascular resection; Venous tumor thrombus.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the ethics committees of Peking University Third Hospital. Informed consent was obtained from all individual participants included in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Lambert EH, Pierorazio PM, Shabsigh A, Olsson CA, Benson MC, McKiernan JM. Prognostic risk stratification and clinical outcomes in patients undergoing surgical treatment for renal cell carcinoma with vascular tumor thrombus. Urology. 2007;69:1054–1058. doi: 10.1016/j.urology.2007.02.052. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
