

A collaborative multiyear, multimodel assessment of seasonal influenza forecasting in the United States
- PMID: 30647115
- PMCID: PMC6386665
- DOI: 10.1073/pnas.1812594116
A collaborative multiyear, multimodel assessment of seasonal influenza forecasting in the United States
Abstract
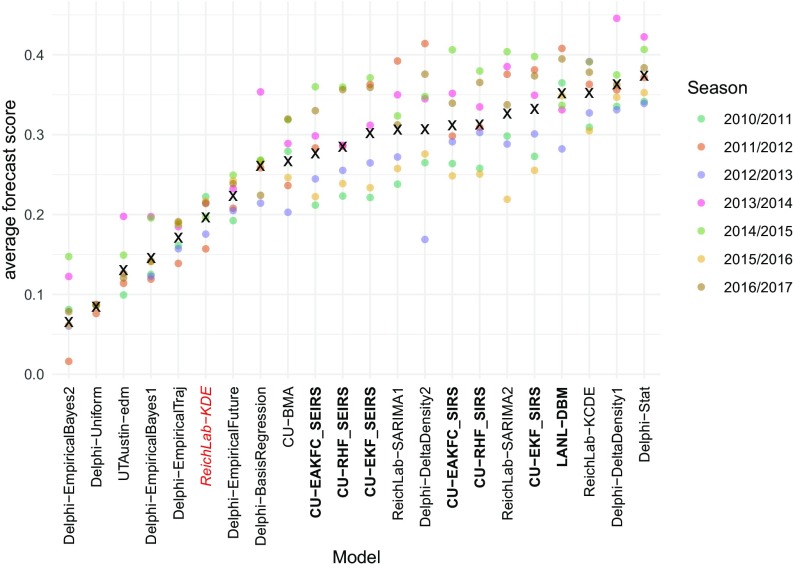
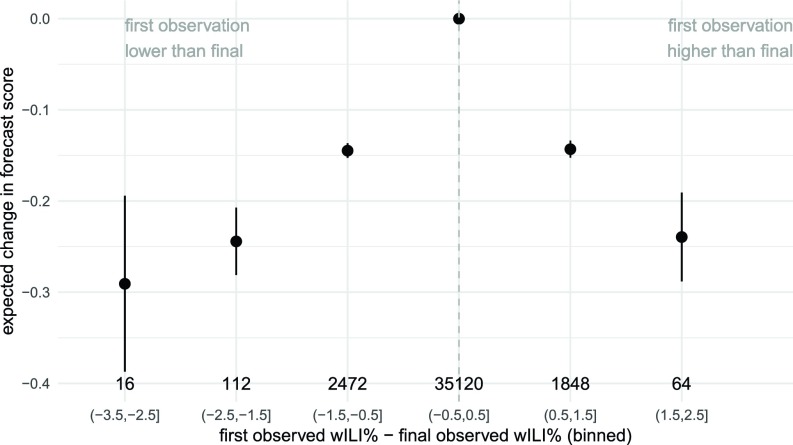
Influenza infects an estimated 9-35 million individuals each year in the United States and is a contributing cause for between 12,000 and 56,000 deaths annually. Seasonal outbreaks of influenza are common in temperate regions of the world, with highest incidence typically occurring in colder and drier months of the year. Real-time forecasts of influenza transmission can inform public health response to outbreaks. We present the results of a multiinstitution collaborative effort to standardize the collection and evaluation of forecasting models for influenza in the United States for the 2010/2011 through 2016/2017 influenza seasons. For these seven seasons, we assembled weekly real-time forecasts of seven targets of public health interest from 22 different models. We compared forecast accuracy of each model relative to a historical baseline seasonal average. Across all regions of the United States, over half of the models showed consistently better performance than the historical baseline when forecasting incidence of influenza-like illness 1 wk, 2 wk, and 3 wk ahead of available data and when forecasting the timing and magnitude of the seasonal peak. In some regions, delays in data reporting were strongly and negatively associated with forecast accuracy. More timely reporting and an improved overall accessibility to novel and traditional data sources are needed to improve forecasting accuracy and its integration with real-time public health decision making.
Keywords: forecasting; infectious disease; influenza; public health; statistics.
Copyright © 2019 the Author(s). Published by PNAS.
Conflict of interest statement
Conflict of interest statement: J.S. and Columbia University disclose partial ownership of SK Analytics.
Figures
Comment in
-
The future of influenza forecasts.Proc Natl Acad Sci U S A. 2019 Feb 19;116(8):2802-2804. doi: 10.1073/pnas.1822167116. Epub 2019 Feb 8. Proc Natl Acad Sci U S A. 2019. PMID: 30737293 Free PMC article. No abstract available.
-
Reply to Bracher: Scoring probabilistic forecasts to maximize public health interpretability.Proc Natl Acad Sci U S A. 2019 Oct 15;116(42):20811-20812. doi: 10.1073/pnas.1912694116. Epub 2019 Sep 26. Proc Natl Acad Sci U S A. 2019. PMID: 31558611 Free PMC article. No abstract available.
-
On the multibin logarithmic score used in the FluSight competitions.Proc Natl Acad Sci U S A. 2019 Oct 15;116(42):20809-20810. doi: 10.1073/pnas.1912147116. Epub 2019 Sep 26. Proc Natl Acad Sci U S A. 2019. PMID: 31558612 Free PMC article. No abstract available.
References
-
- World Health Organization 2016 Anticipating emerging infectious disease epidemics (World Health Organization, Geneva). Available at http://apps.who.int/iris/bitstream/handle/10665/252646/WHO-OHE-PED-2016..... Accessed January 25, 2018.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
