

Left ventricular outflow tract obstruction following aortic valve replacement: A review of risk factors, mechanism, and management
- PMID: 30648672
- PMCID: PMC6350428
- DOI: 10.4103/aca.ACA_226_17
Left ventricular outflow tract obstruction following aortic valve replacement: A review of risk factors, mechanism, and management
Abstract
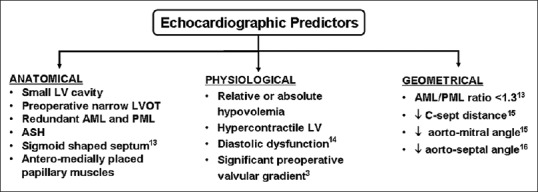
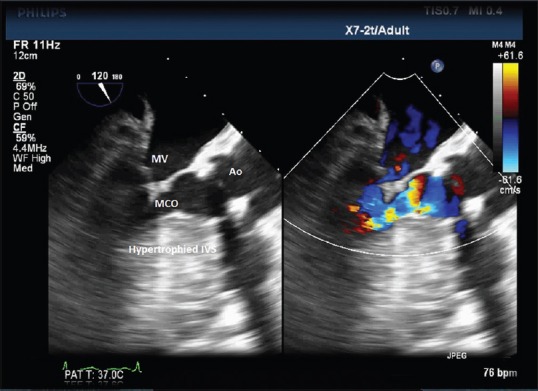
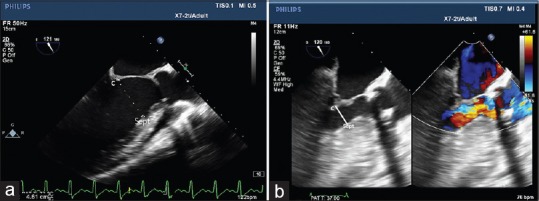
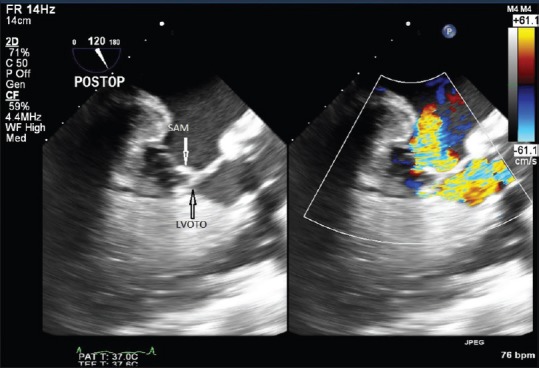
The presence of dynamic left ventricular outflow tract obstruction (LVOTO) can complicate the postoperative course of patients undergoing surgical aortic valve replacement (AVR). The phenomenon of LVOTO is a consequence of an interplay of various pathoanatomic mechanisms. The prevailing cardiovascular milieu dictates the hemodynamic significance of the resultant LVOTO in addition to the anatomical risk factors. A thorough understanding of the predisposing factors, mechanism, and hemodynamic sequel of the obstruction is pivotal in managing these cases. A comprehensive echocardiographic examination aids in risk prediction, diagnosis, severity characterization, and follow-up of management efficacy in the setting of postoperative LVOTO. The armamentarium of management modalities includes conservative (medical) and surgical options. A stepwise approach should be formulated based on the physiological and anatomical substrates predisposing to LVOTO. The index phenomenon occurs more frequently than appreciated and should be considered when the post-AVR patients exhibit hemodynamic instability unresponsive to conventional supportive measures. The present article provides an overview of various peculiarities of this under-recognized phenomenon in the context of the perioperative management of patients undergoing AVR.
Keywords: Aortic valve replacement; asymmetrical septal hypertrophy; left ventricular outflow tract obstruction; mitral systolic anterior motion.
Conflict of interest statement
None
Figures
Similar articles
-
Novel Multiphase Assessment for Predicting Left Ventricular Outflow Tract Obstruction Before Transcatheter Mitral Valve Replacement.JACC Cardiovasc Interv. 2019 Dec 9;12(23):2402-2412. doi: 10.1016/j.jcin.2019.06.015. Epub 2019 Oct 16. JACC Cardiovasc Interv. 2019. PMID: 31629753
-
How Would We Treat Our Own Left Ventricular Outflow Tract Obstruction in Transcatheter Mitral Valve Replacement?J Cardiothorac Vasc Anesth. 2025 Jun;39(6):1401-1413. doi: 10.1053/j.jvca.2025.02.019. Epub 2025 Feb 18. J Cardiothorac Vasc Anesth. 2025. PMID: 40074585 Review.
-
Left Ventricular Outflow Tract Obstruction From Preserved Leaflet After Mitral Valve Replacement.Ann Thorac Surg. 2020 Jul;110(1):e15-e17. doi: 10.1016/j.athoracsur.2019.10.074. Epub 2019 Dec 18. Ann Thorac Surg. 2020. PMID: 31863759
-
Left ventricular outflow tract obstruction after mitral valve repair. Results of the sliding leaflet technique.Circulation. 1993 Nov;88(5 Pt 2):II30-4. Circulation. 1993. PMID: 8222170
-
Left ventricular outflow tract obstruction after bioprosthetic mitral valve replacement with preservation of the anterior leaflet.Rev Cardiovasc Med. 2011;12(1):48-51. doi: 10.3909/ricm0556. Rev Cardiovasc Med. 2011. PMID: 21546891 Review.
Cited by
-
Percutaneous Intramyocardial Septal Radiofrequency Ablation in Patients With Drug-Refractory Hypertrophic Obstructive Cardiomyopathy.JAMA Cardiol. 2022 May 1;7(5):529-538. doi: 10.1001/jamacardio.2022.0259. JAMA Cardiol. 2022. PMID: 35353129 Free PMC article. Clinical Trial.
-
How to Image and Manage Prosthesis-Related Complications After Transcatheter Aortic Valve Replacement.Curr Cardiol Rep. 2021 Jul 1;23(8):94. doi: 10.1007/s11886-021-01522-2. Curr Cardiol Rep. 2021. PMID: 34196775 Review.
-
Conservative Management of Suicide Left Ventricle After Surgical Aortic Valve Replacement.Cureus. 2023 Aug 3;15(8):e42890. doi: 10.7759/cureus.42890. eCollection 2023 Aug. Cureus. 2023. PMID: 37664339 Free PMC article.
-
A case report of ventricular suicide following transcatheter aortic valve replacement for severe aortic stenosis in a patient with hypertrophic cardiomyopathy: the danger of abrupt afterload reduction.Egypt Heart J. 2025 Jun 1;77(1):52. doi: 10.1186/s43044-025-00650-2. Egypt Heart J. 2025. PMID: 40451985 Free PMC article.
-
Outcomes of transcatheter aortic valve replacement in patients with hypertrophic cardiomyopathy: a systematic review.Ann Transl Med. 2025 Feb 28;13(1):6. doi: 10.21037/atm-24-41. Epub 2025 Feb 25. Ann Transl Med. 2025. PMID: 40115067 Free PMC article. Review.
References
-
- Bach DS. Subvalvular left ventricular outflow obstruction for patients undergoing aortic valve replacement for aortic stenosis: Echocardiographic recognition and identification of patients at risk. J Am Soc Echocardiogr. 2005;18:1155–62. - PubMed
-
- Aurigemma G, Battista S, Orsinelli D, Sweeney A, Pape L, Cuénoud H, et al. Abnormal left ventricular intracavitary flow acceleration in patients undergoing aortic valve replacement for aortic stenosis. A marker for high postoperative morbidity and mortality. Circulation. 1992;86:926–36. - PubMed
-
- Tewari P, Basu R. Left ventricular outflow tract obstruction after mitral valve replacement. Anesth Analg. 2008;106:65–6. - PubMed
-
- Bartunek J, Sys SU, Rodrigues AC, van Schuerbeeck E, Mortier L, de Bruyne B, et al. Abnormal systolic intraventricular flow velocities after valve replacement for aortic stenosis. Mechanisms, predictive factors, and prognostic significance. Circulation. 1996;93:712–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical