

Association Between Postoperative Delirium and Long-term Cognitive Function After Major Nonemergent Surgery
- PMID: 30649138
- PMCID: PMC6484789
- DOI: 10.1001/jamasurg.2018.5093
Association Between Postoperative Delirium and Long-term Cognitive Function After Major Nonemergent Surgery
Abstract
Importance: Postoperative delirium is associated with decreases in long-term cognitive function in elderly populations.
Objective: To determine whether postoperative delirium is associated with decreased long-term cognition in a younger, more heterogeneous population.
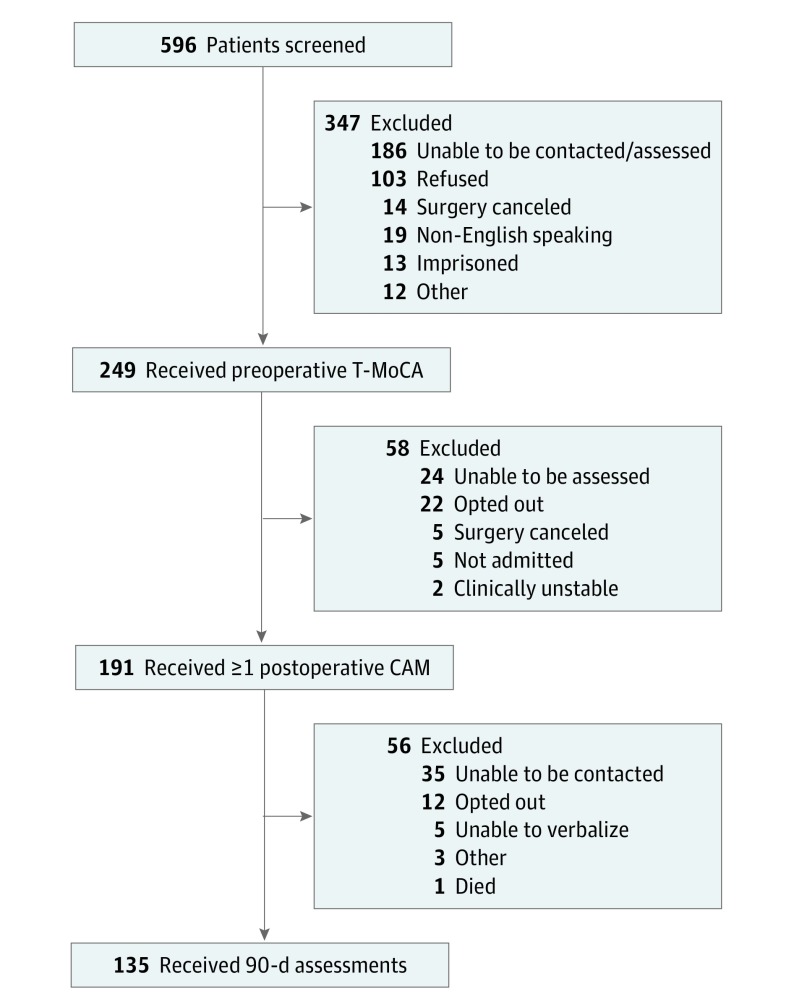
Design, setting, and participants: A prospective cohort study was conducted at a single academic medical center (≥800 beds) in the southeastern United States from September 5, 2017, through January 15, 2018. A total of 191 patients aged 18 years or older who were English-speaking and were anticipated to require at least 1 night of hospital admission after a scheduled major nonemergent surgery were included. Prisoners, individuals without baseline cognitive assessments, and those who could not provide informed consent were excluded. Ninety-day follow-up assessments were performed on 135 patients (70.7%).
Exposures: The primary exposure was postoperative delirium defined as any instance of delirium occurring 24 to 72 hours after an operation. Delirium was diagnosed by the research team using the Confusion Assessment Method (CAM).
Main outcomes and measures: The primary outcome was change in cognition at 90 days after surgery compared with baseline, preoperative cognition. Cognition was measured using a telephone version of the Montreal Cognitive Assessment (T-MoCA) with cognitive impairment defined as a score less than 18 on a scale of 0 to 22.
Results: Of the 191 patients included in the study, 110 (57.6%) were women; the mean (SD) age was 56.8 (16.7) years. For the primary outcome of interest, patients with and without delirium had a small increase in T-MoCA scores at 90 days compared with baseline on unadjusted analysis (with delirium, 0.69; 95% CI, -0.34 to 1.73 vs without delirium, 0.67; 95% CI, 0.17-1.16). The initial multivariate linear regression model included age, preoperative American Society of Anesthesiologists Physical Status Classification System score, preoperative cognitive impairment, and duration of anesthesia. Preoperative cognitive impairment proved to be the only notable confounder: when adjusted for preoperative cognitive impairment, patients with delirium had a 0.70-point greater decrease in 90-day T-MoCA scores than those without delirium compared with their respective baseline scores (with delirium, 0.16; 95% CI, -0.63 to 0.94 vs without delirium, 0.86; 95% CI, 0.40-1.33).
Conclusions and relevance: Although a statistically significant association between 90-day cognition and postoperative delirium was not noted, patients with preoperative cognitive impairment appeared to have improvements in cognition 90 days after surgery; however, this finding was attenuated if they became delirious. Preoperative cognitive impairment alone should not preclude patients from undergoing indicated surgical procedures.
Conflict of interest statement
Figures
Comment in
-
Challenges With Postoperative Cognitive Impairment Research.JAMA Surg. 2019 Apr 1;154(4):334-335. doi: 10.1001/jamasurg.2018.5110. JAMA Surg. 2019. PMID: 30649134 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
