

Effect of prenatal calcium supplementation on bone during pregnancy and 1 y postpartum
- PMID: 30649176
- PMCID: PMC6900564
- DOI: 10.1093/ajcn/nqy233
Effect of prenatal calcium supplementation on bone during pregnancy and 1 y postpartum
Abstract
Background: Low calcium intake during pregnancy may cause maternal skeletal calcium mobilization to meet fetal needs. The Recommended Dietary Allowance (RDA) for calcium in nonpregnant, pregnant, or lactating women aged 19-50 y is 1000 mg/d; most women in the United States report consuming 60-80% of the calcium RDA. An insufficient calcium intake could increase maternal bone loss during pregnancy and reduce bone recovery postpartum.
Objectives: The aim of this study was to determine the effect of maternal calcium supplementation on peripheral cortical and trabecular bone loss during pregnancy and bone gain postpartum.
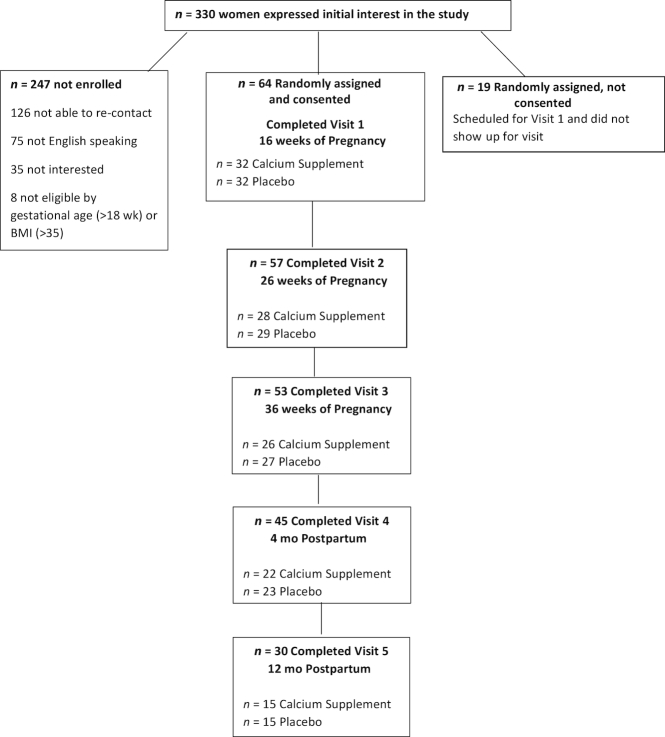
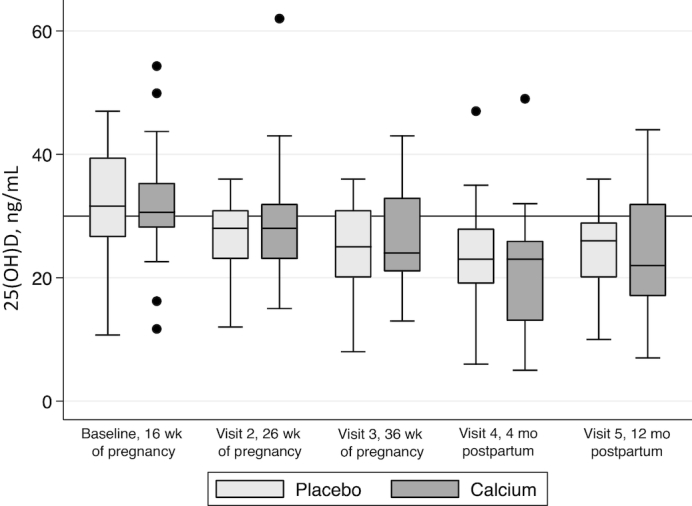
Methods: A total of 64 women were enrolled in the study at 16 wk of gestation and randomly assigned to receive 1000 mg Ca/d or placebo for the remainder of the pregnancy. Measurements were performed at 16, 26, and 36 wk of pregnancy and at 4 and 12 mo postpartum for serum 25-hydroxyvitamin D and markers of bone turnover. Trabecular and cortical bone mineral density (BMD) and content were assessed at the tibia and radius by peripheral quantitative computed tomography.
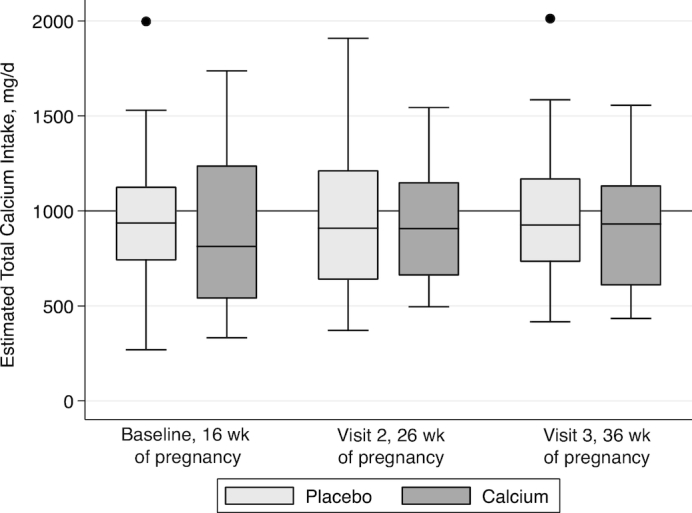
Results: Mean ± SD daily calcium intake at baseline was 733 ± 350 mg; only 25% of the women met the RDA. Thirty women (47% of those enrolled) remained in the study at 12 mo postpartum. After controlling for baseline bone value, serum 25-hydroxyvitamin D concentrations, length of breastfeeding, and body mass index, the calcium group had significantly greater increases in radial total BMD (P = 0.02) and tibial cortical BMD (P = 0.03) at 12 mo postpartum than the placebo group. Trabecular and total BMD at the tibia trended toward higher values (P < 0.06) in the calcium group than in the placebo group in the same models.
Conclusions: These data show that supplemental calcium provided during pregnancy may improve bone recovery postpartum in women consuming a typical US diet. A larger study is warranted to solidify the conclusions. This trial was registered at clinicaltrials.gov as NCT01145573.
Figures
Comment in
-
The quest for evidence for calcium requirements for bone during pregnancy and lactation.Am J Clin Nutr. 2019 Jan 1;109(1):3-4. doi: 10.1093/ajcn/nqy335. Am J Clin Nutr. 2019. PMID: 30668614 No abstract available.
References
-
- Institute of Medicine. Dietary Reference Intakes for calcium, phosphorus, magnesium, vitamin D, and fluoride. Washington (DC):National Academies Press; 1997. - PubMed
-
- Institute of Medicine (IOM). Dietary Reference Intakes for calcium and vitamin D. Washington (DC): National Academies Press; 2011. - PubMed
-
- Kalkwarf HJ, Specker BL, Heubi JE, Vieira NE, Yergey AL. Intestinal calcium absorption of women during lactation and after weaning. Am J Clin Nutr. 1996;63(4):526–31. - PubMed
-
- Cross NA, Hillman LS, Allen SH, Krause GF, Vieira NE. Calcium homeostasis and bone metabolism during pregnancy, lactation, and postweaning: a longitudinal study. Am J Clin Nutr. 1995;61(3):514–23. - PubMed
-
- Ritchie LD, Fung EB, Halloran BP, Turnlund JR, Van Loan MD, Cann CE, King JC. A longitudinal study of calcium homeostasis during human pregnancy and lactation and after resumption of menses. Am J Clin Nutr. 1998;67(4):693–701. - PubMed
