

Evaluation of Antibody Properties and Clinically Relevant Immunogenicity, Anaphylaxis, and Hypersensitivity Reactions in Two Phase III Trials of Tralokinumab in Severe, Uncontrolled Asthma
- PMID: 30649752
- PMCID: PMC6520328
- DOI: 10.1007/s40264-018-00788-w
Evaluation of Antibody Properties and Clinically Relevant Immunogenicity, Anaphylaxis, and Hypersensitivity Reactions in Two Phase III Trials of Tralokinumab in Severe, Uncontrolled Asthma
Abstract
Introduction: Tralokinumab is a monoclonal antibody (mAb) that neutralizes interleukin (IL)-13, a cytokine involved in the pathogenesis of asthma.
Objective: The objectives of this study were to characterize the potential immunogenic properties of tralokinumab and report data for anti-drug antibodies (ADAs) and hypersensitivity reactions from two phase III clinical trials.
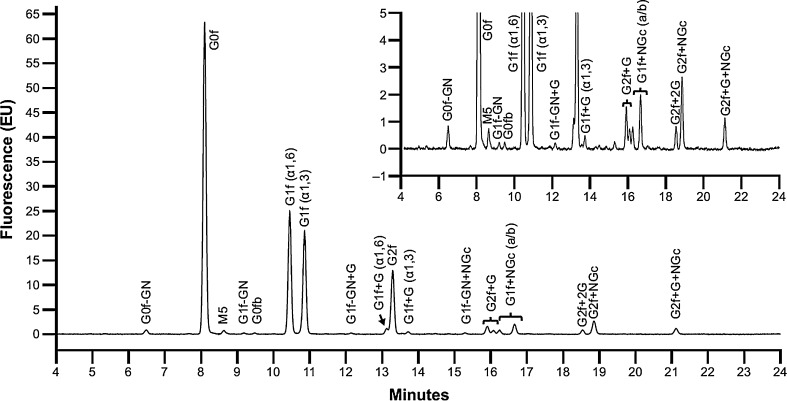
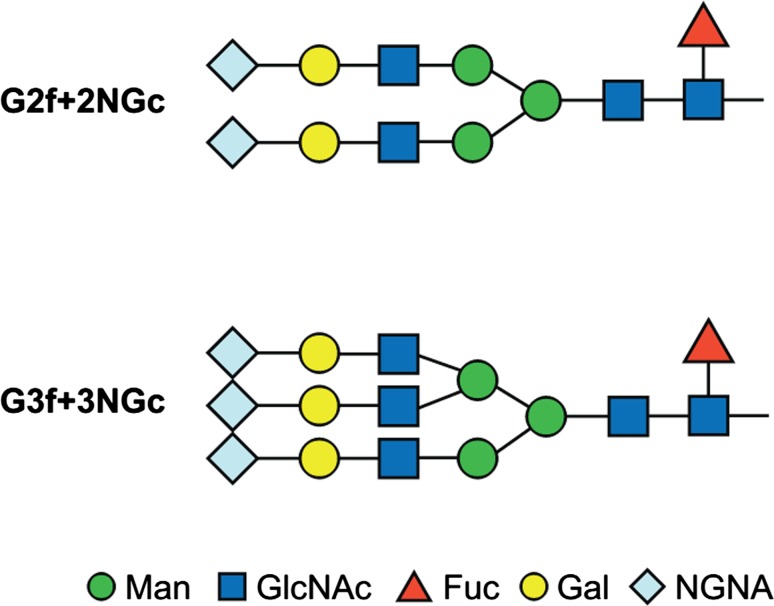
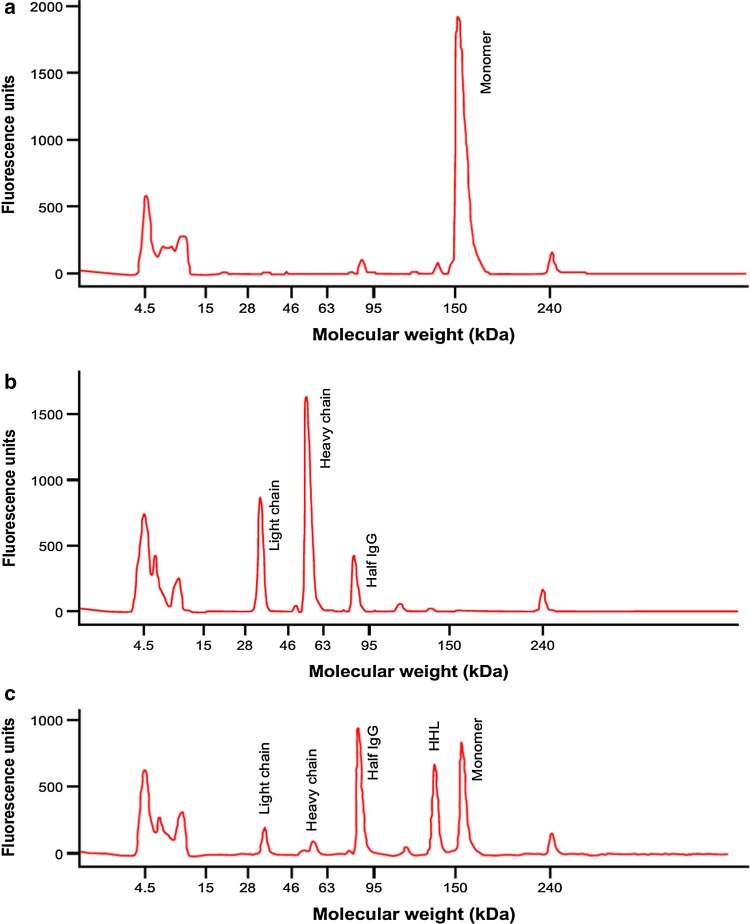
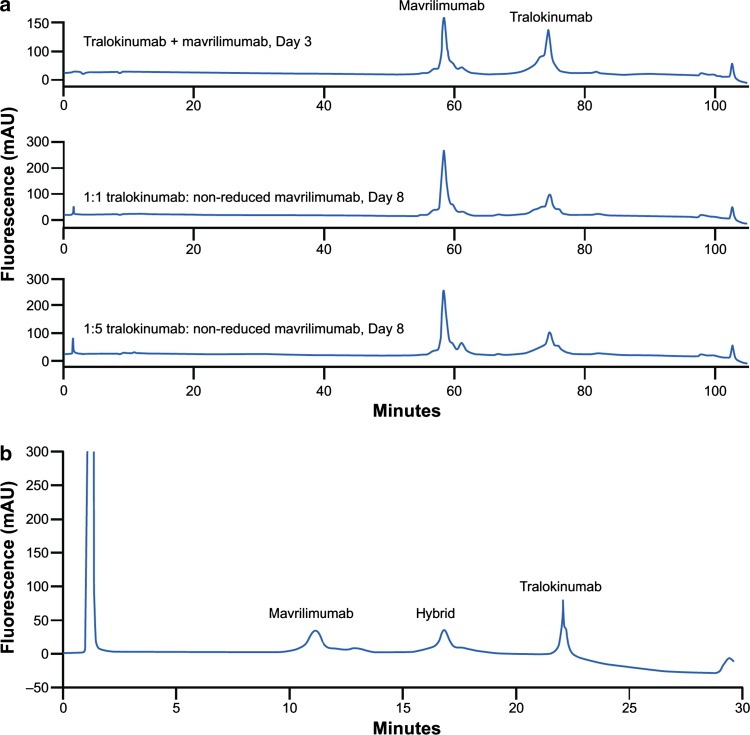
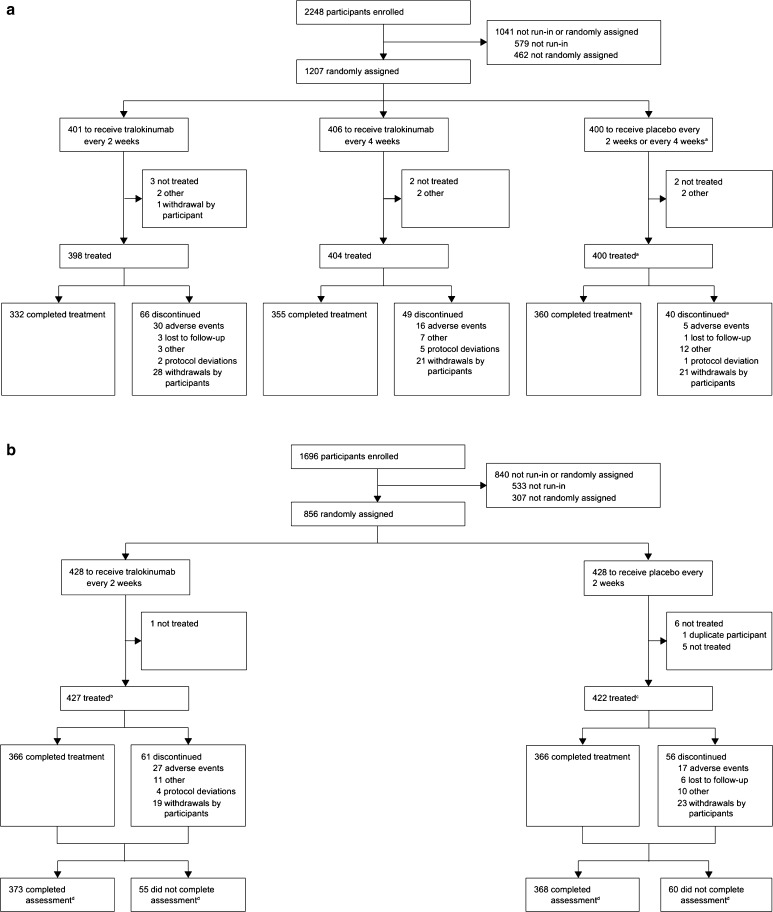
Methods: The oligosaccharide structure of tralokinumab, Fab-arm exchange, and ADAs were characterized by standard techniques. Hypersensitivity adverse events (AEs) were evaluated in two pivotal clinical trials of tralokinumab in severe, uncontrolled asthma: STRATOS 1 and 2 (NCT02161757 and NCT02194699).
Results: No galactose-α-1,3-galactose (α-Gal) epitopes were found in the Fab region of tralokinumab and only 4.5% of glycoforms contained α-Gal in the Fc region. Under non-reducing conditions, Fab-arm exchange did not take place with another immunoglobulin (Ig) G4 mAb (mavrilimumab). However, following glutathione reduction, a hybrid antibody with monovalent bioactivity was detected. ADA incidences (titers) were as follows: STRATOS 1-every 2 weeks (Q2 W) 0.8% (26.0), every 4 weeks (Q4 W) 0.5% (26.0), placebo 0.8% (52.0); STRATOS 2-Q2 W 1.2% (39.0), placebo 0.8% (13.0). Participant-reported hypersensitivity AE rates were as follows: STRATOS 1-Q2 W 25.9%, Q4 W 25.0%, placebo 25.5%; STRATOS 2-Q2 W 13.2%, placebo 9.0%. External evaluation for anaphylaxis by Sampson criteria found no tralokinumab-related severe hypersensitivity or anaphylaxis reactions.
Conclusion: Preclinical assessments suggested a low likelihood of immunogenicity for tralokinumab. In STRATOS 1 and 2, ADA incidence was low, no differences were found between tralokinumab-treated and placebo groups in reporting of hypersensitivity reactions, and there were no Sampson criteria-evaluated anaphylaxis events with tralokinumab treatment. Together, the results suggest that tralokinumab treatment would not increase the risk for severe hypersensitivity or anaphylactic reactions.
Conflict of interest statement
Conflicts of interest
Yuling Li was an employee of MedImmune, the biologics division of AstraZeneca, at the time the study took place; her current affiliation is CBT Pharmaceuticals. Jihong Wang and Weichen Xu are employees of MedImmune, the biologics division of AstraZeneca. Nicholas White is an employee of MedImmune and an AstraZeneca shareholder. Mats Carlsson, Martin Braddock, and Ayman Megally are employees of AstraZeneca, the sponsor of STRATOS 1 and STRATOS 2. Gene Colice is an employee of and holds stock options in AstraZeneca. Gillian Hunter is a consultant employed by AstraZeneca.
Ethical approval and informed consent
STRATOS 1 and STRATOS 2 were performed in accordance with the ethical principles that have their origin in the Declaration of Helsinki and that are consistent with International Conference on Harmonisation (ICH)/Good Clinical Practice (GCP), applicable regulatory requirements, and the AstraZeneca policy on Bioethics. All participating centers obtained approval from an independent ethics committee and all participants provided written informed consent.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
