

Tumor-Infiltrating Lymphocytes and Prognosis: A Pooled Individual Patient Analysis of Early-Stage Triple-Negative Breast Cancers
- PMID: 30650045
- PMCID: PMC7010425
- DOI: 10.1200/JCO.18.01010
Tumor-Infiltrating Lymphocytes and Prognosis: A Pooled Individual Patient Analysis of Early-Stage Triple-Negative Breast Cancers
Abstract
Purpose: The aim of the current study was to conduct a pooled analysis of studies that have investigated the prognostic value of tumor-infiltrating lymphocytes (TILs) in early-stage triple negative breast cancer (TNBC).
Methods: Participating studies had evaluated the percentage infiltration of stromally located TILs (sTILs) that were quantified in the same manner in patient diagnostic samples of early-stage TNBC treated with anthracycline-based chemotherapy with or without taxanes. Cox proportional hazards regression models stratified by trial were used for invasive disease-free survival (iDFS; primary end point), distant disease-free survival (D-DFS), and overall survival (OS), fitting sTILs as a continuous variable adjusted for clinicopathologic factors.
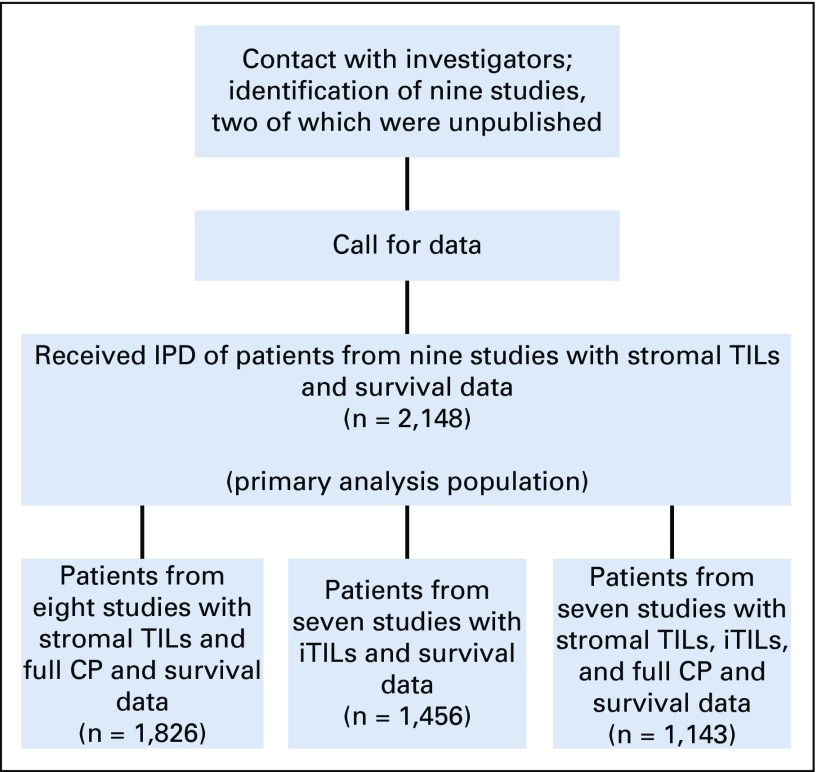
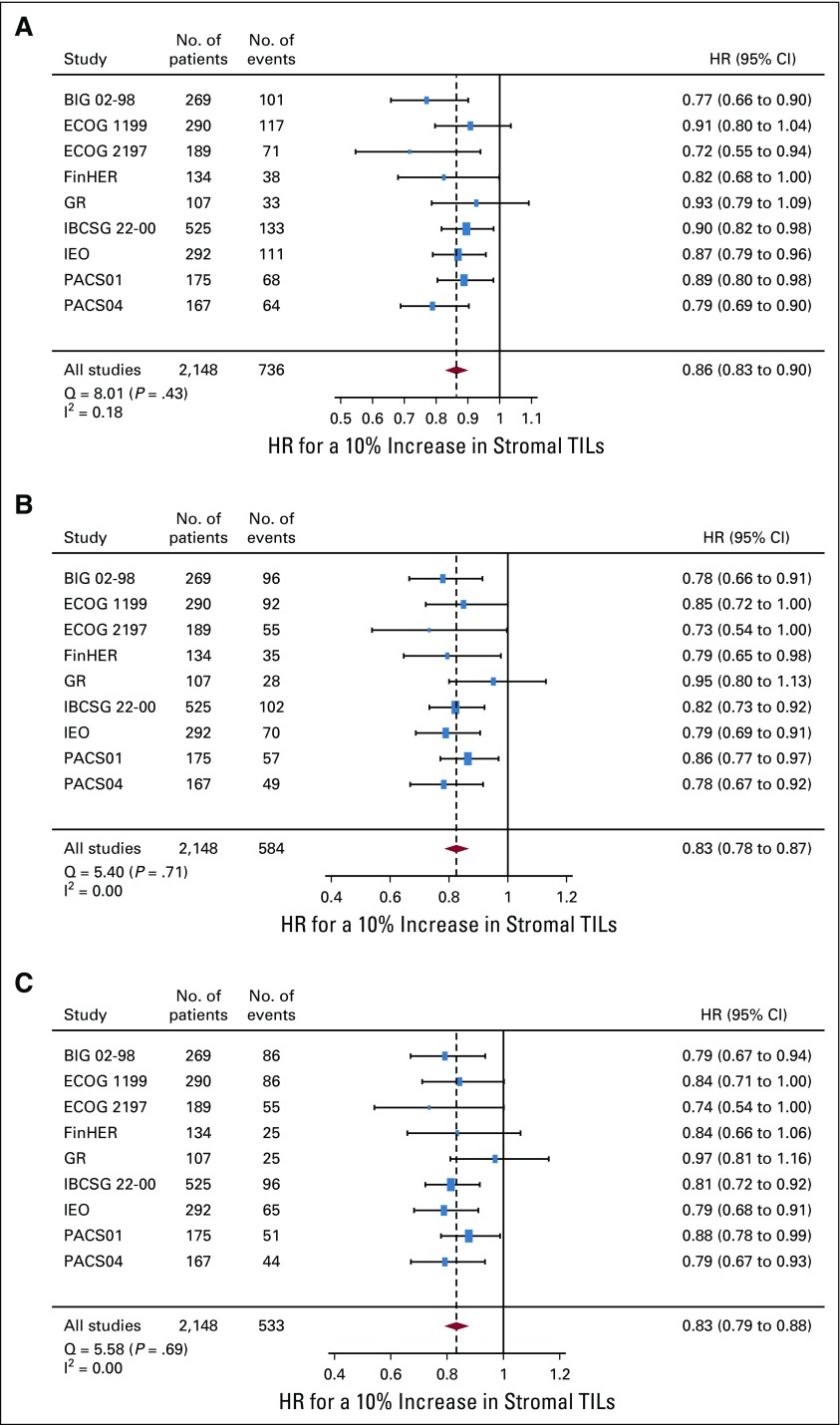
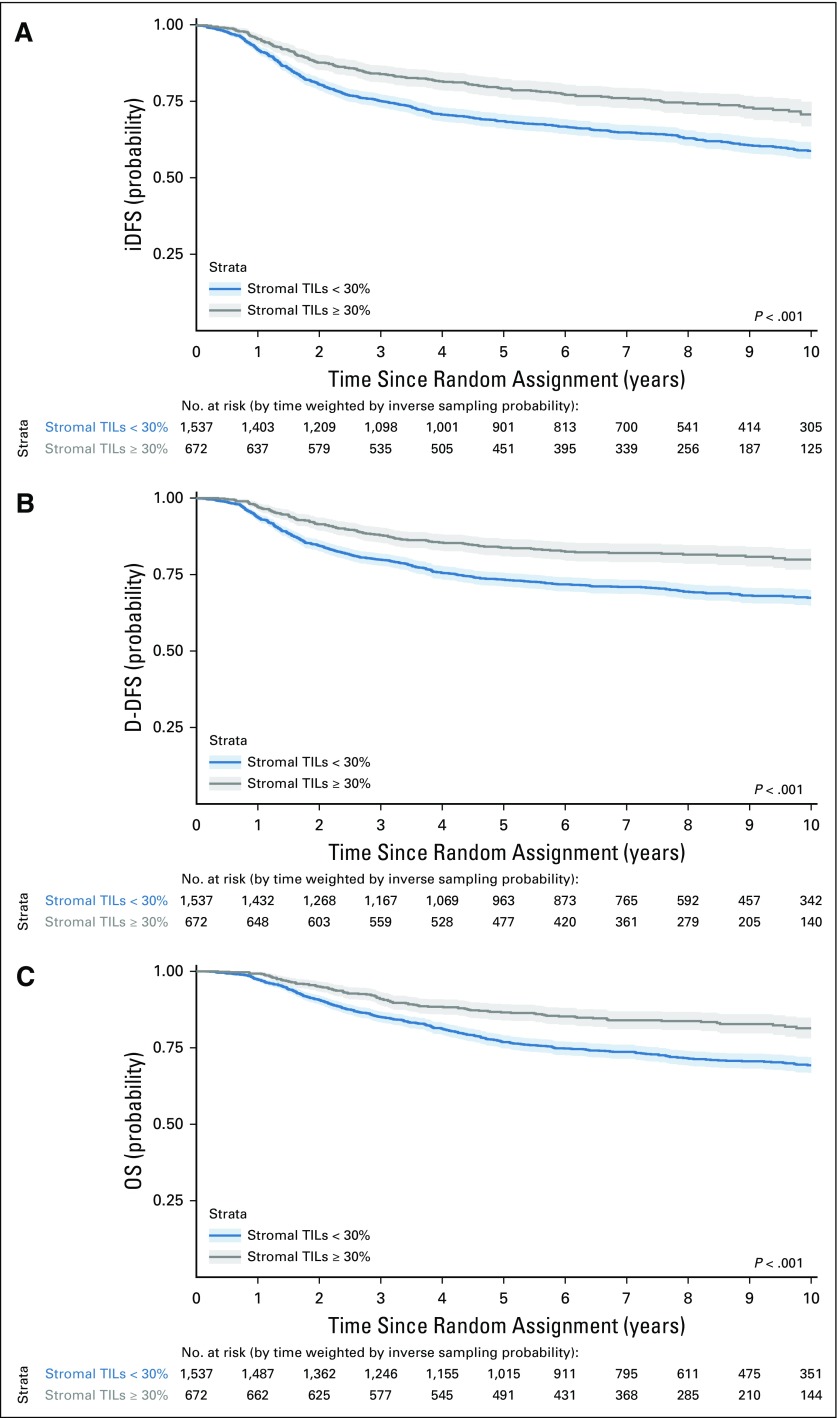
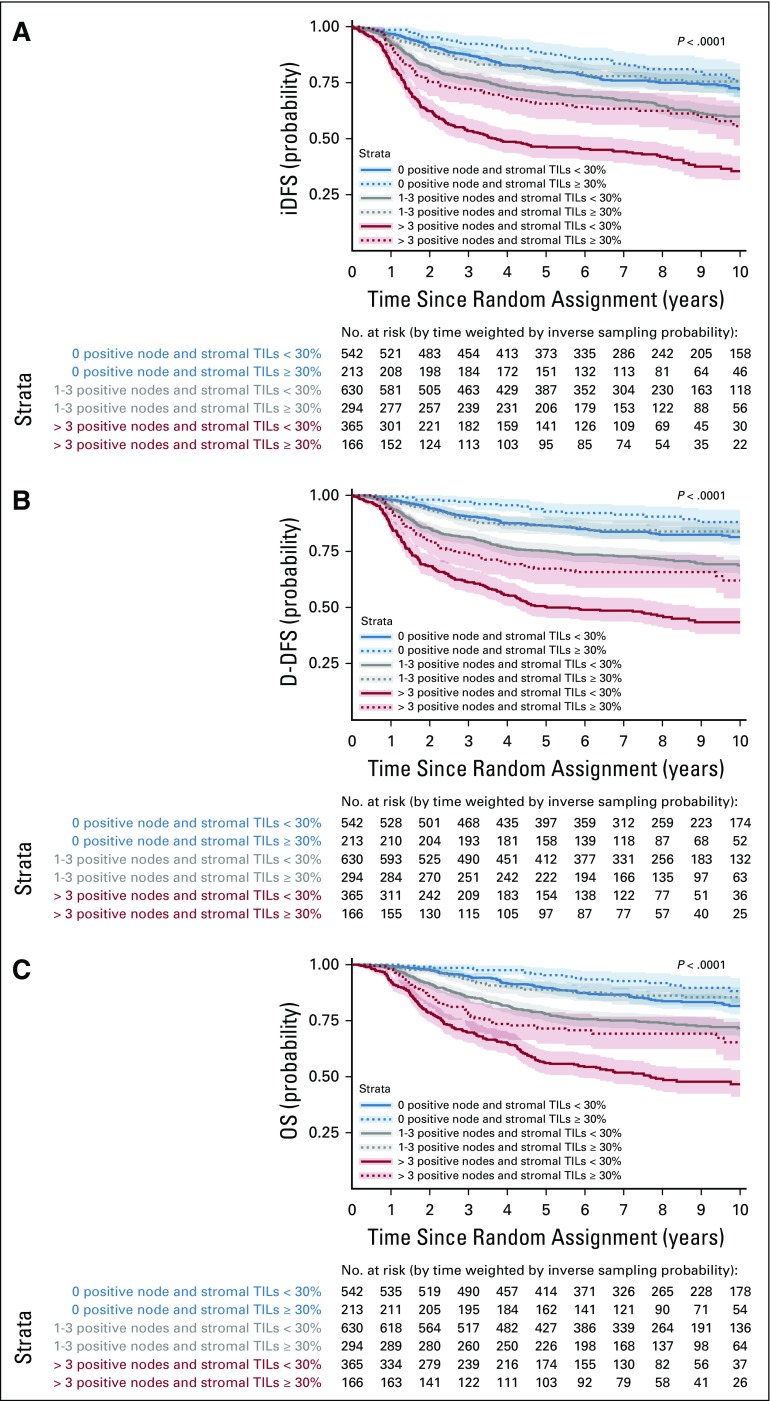
Results: We collected individual data from 2,148 patients from nine studies. Average age was 50 years (range, 22 to 85 years), and 33% of patients were node negative. The average value of sTILs was 23% (standard deviation, 20%), and 77% of patients had 1% or more sTILs. sTILs were significantly lower with older age ( P = .001), larger tumor size ( P = .01), more nodal involvement ( P = .02), and lower histologic grade ( P = .001). A total of 736 iDFS and 548 D-DFS events and 533 deaths were observed. In the multivariable model, sTILs added significant independent prognostic information for all end points (likelihood ratio χ2, 48.9 iDFS; P < .001; χ2, 55.8 D-DFS; P < .001; χ2, 48.5 OS; P < .001). Each 10% increment in sTILs corresponded to an iDFS hazard ratio of 0.87 (95% CI, 0.83 to 0.91) for iDFS, 0.83 (95% CI, 0.79 to 0.88) for D-DFS, and 0.84 (95% CI, 0.79 to 0.89) for OS. In node-negative patients with sTILs ≥ 30%, 3-year iDFS was 92% (95% CI, 89% to 98%), D-DFS was 97% (95% CI, 95% to 99%), and OS was 99% (95% CI, 97% to 100%).
Conclusion: This pooled data analysis confirms the strong prognostic role of sTILs in early-stage TNBC and excellent survival of patients with high sTILs after adjuvant chemotherapy and supports the integration of sTILs in a clinicopathologic prognostic model for patients with TNBC. This model can be found at www.tilsinbreastcancer.org .
Figures
References
-
- Savas P, Salgado R, Denkert C, et al. Clinical relevance of host immunity in breast cancer: From TILs to the clinic. Nat Rev Clin Oncol. 2016;13:228–241. - PubMed
-
- Denkert C, Wienert S, Poterie A, et al. Standardized evaluation of tumor-infiltrating lymphocytes in breast cancer: Results of the ring studies of the international immuno-oncology biomarker working group. Mod Pathol. 2016;29:1155–1164. - PubMed
-
- American Joint Committee on Cancer BreastinHortobagyi GN, Connolly JL, D’Orsi CJ.(eds)AJCC Cancer Staging Manual ed 8New York, NY: Springer; 2017
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
