

Effect of a Multidimensional Physical Activity Intervention on Body Mass Index, Skinfolds and Fitness in South African Children: Results from a Cluster-Randomised Controlled Trial
- PMID: 30650624
- PMCID: PMC6352127
- DOI: 10.3390/ijerph16020232
Effect of a Multidimensional Physical Activity Intervention on Body Mass Index, Skinfolds and Fitness in South African Children: Results from a Cluster-Randomised Controlled Trial
Abstract
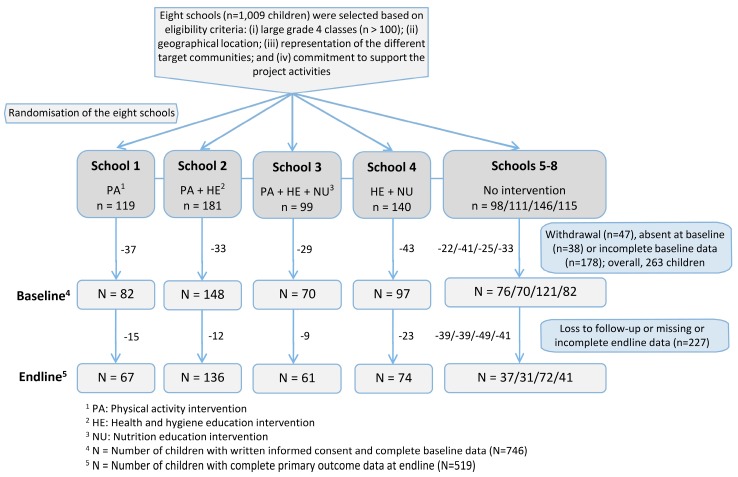
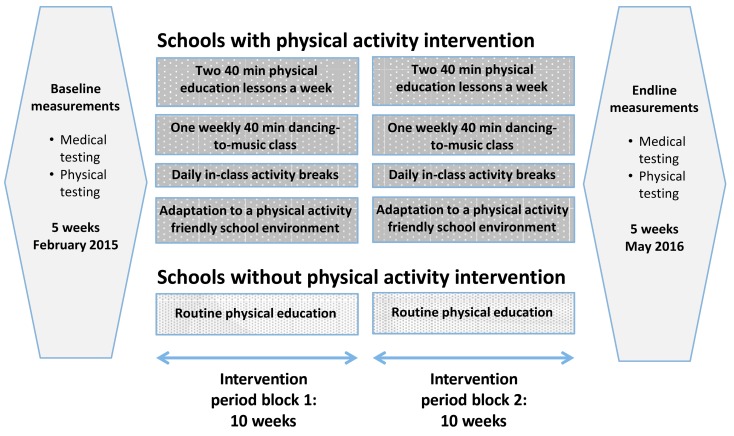
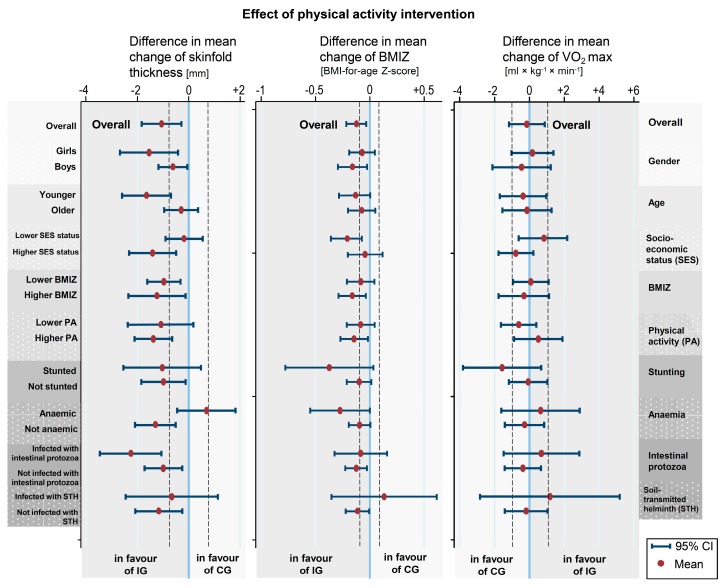
Obesity-related conditions impose a considerable and growing burden on low- and middle-income countries, including South Africa. We aimed to assess the effect of twice a 10-week multidimensional, school-based physical activity intervention on children's health in Port Elizabeth, South Africa. A cluster-randomised controlled trial was implemented from February 2015 to May 2016 in grade 4 classes in eight disadvantaged primary schools. Interventions consisted of physical education lessons, moving-to-music classes, in-class activity breaks and school infrastructure enhancement to promote physical activity. Primary outcomes included cardiorespiratory fitness, body mass index (BMI) and skinfold thickness. Explanatory variables were socioeconomic status, self-reported physical activity, stunting, anaemia and parasite infections. Complete data were available from 746 children. A significantly lower increase in the mean BMI Z-score (estimate of difference in mean change: -0.17; 95% confidence interval (CI): -0.24 to -0.09; p < 0.001) and reduced increase in the mean skinfold thickness (difference in mean change: -1.06; 95% CI: -1.83 to -0.29; p = 0.007) was observed in intervention schools. No significant group difference occurred in the mean change of cardiorespiratory fitness (p > 0.05). These findings show that a multidimensional, school-based physical activity intervention can reduce the increase in specific cardiovascular risk factors. However, a longer and more intensive intervention might be necessary to improve cardiorespiratory fitness.
Keywords: South Africa; body mass index; cardiorespiratory fitness; intestinal protozoa; physical activity programme; school-aged children; soil-transmitted helminths.
Conflict of interest statement
All authors declare no competing interests.
Figures
Comment in
-
JPEN Journal Club 45. Cluster Randomization.JPEN J Parenter Enteral Nutr. 2019 Sep;43(7):941-943. doi: 10.1002/jpen.1598. Epub 2019 Apr 22. JPEN J Parenter Enteral Nutr. 2019. PMID: 31006871 No abstract available.
References
-
- Lim S.S., Vos T., Flaxman A.D., Danaei G., Shibuya K., Adair-Rohani H., Amann M., Anderson H.R., Andrews K.G., Aryee M., et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2224–2260. doi: 10.1016/S0140-6736(12)61766-8. - DOI - PMC - PubMed
-
- Ekelund U., Sardinha L.B., Anderssen S.A., Harro M., Franks P.W., Brage S., Cooper A.R., Andersen L.B., Riddoch C., Froberg K. Associations between objectively assessed physical activity and indicators of body fatness in 9- to 10-y-old European children: A population-based study from 4 distinct regions in Europe (the European Youth Heart Study) Am. J. Clin. Nutr. 2004;80:584–590. doi: 10.1093/ajcn/80.3.584. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
