

Relative Impact of Right Ventricular Electromechanical Dyssynchrony Versus Pulmonary Regurgitation on Right Ventricular Dysfunction and Exercise Intolerance in Patients After Repair of Tetralogy of Fallot
- PMID: 30651018
- PMCID: PMC6497336
- DOI: 10.1161/JAHA.118.010903
Relative Impact of Right Ventricular Electromechanical Dyssynchrony Versus Pulmonary Regurgitation on Right Ventricular Dysfunction and Exercise Intolerance in Patients After Repair of Tetralogy of Fallot
Abstract
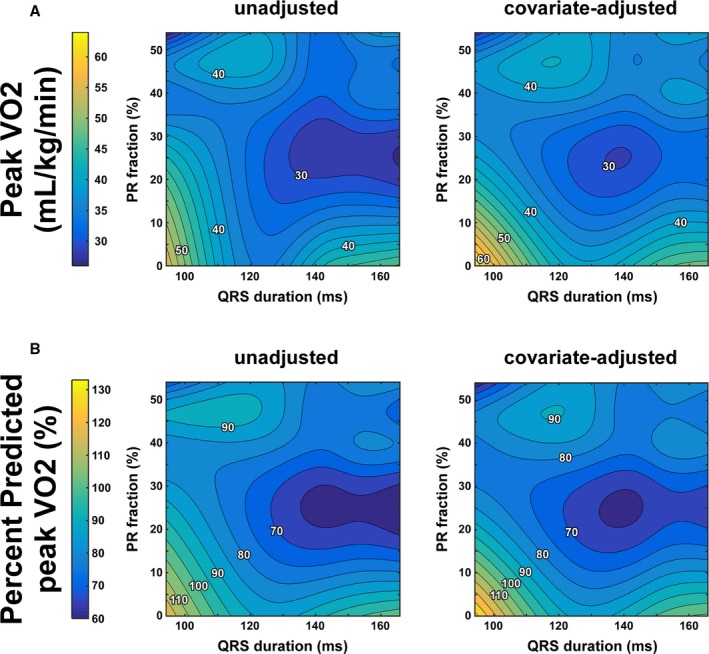
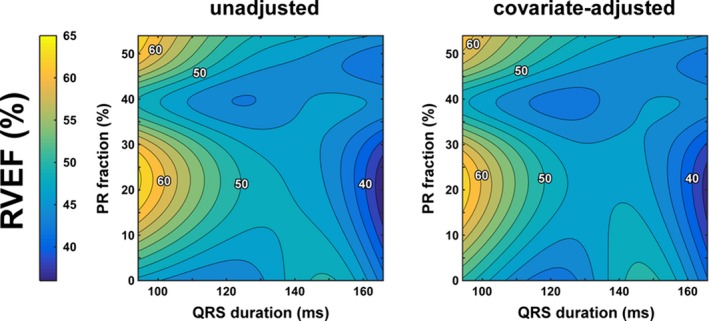
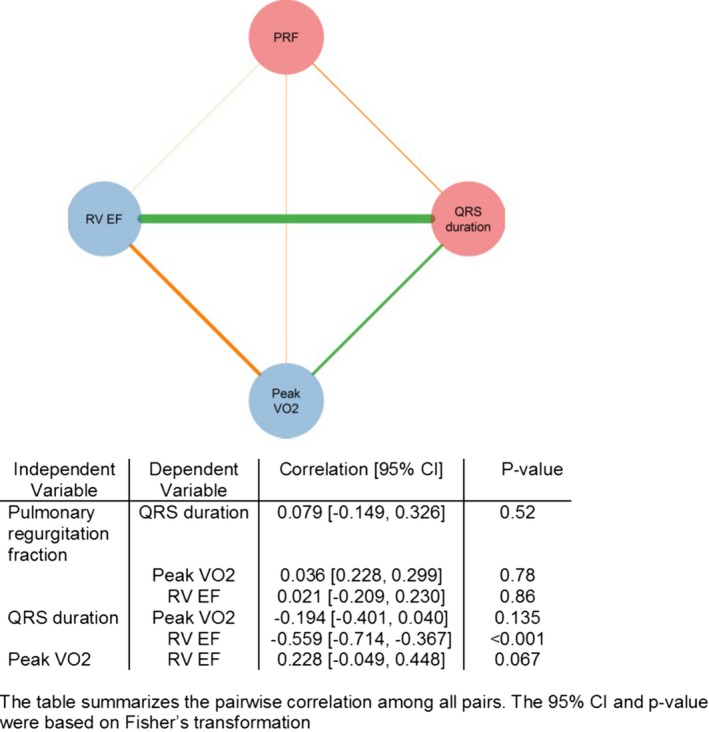
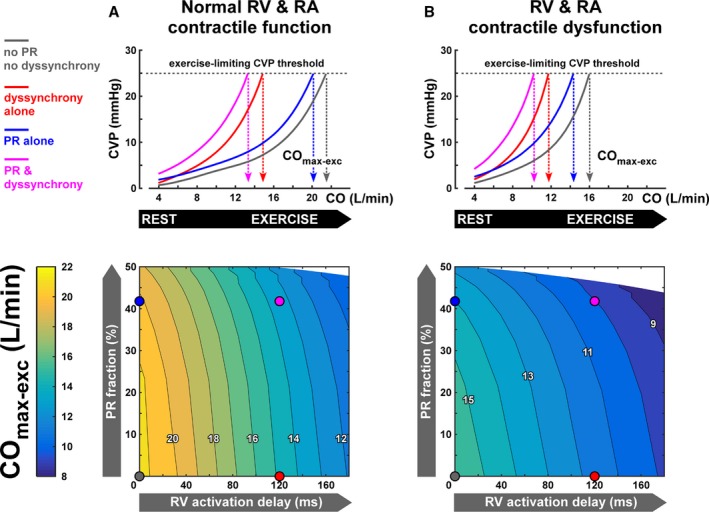
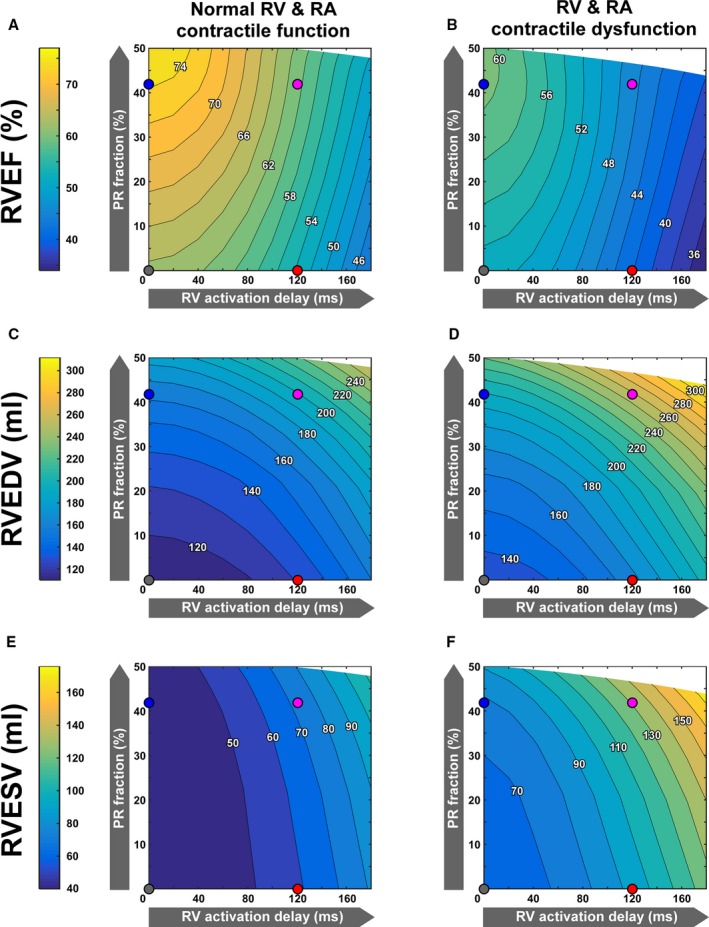
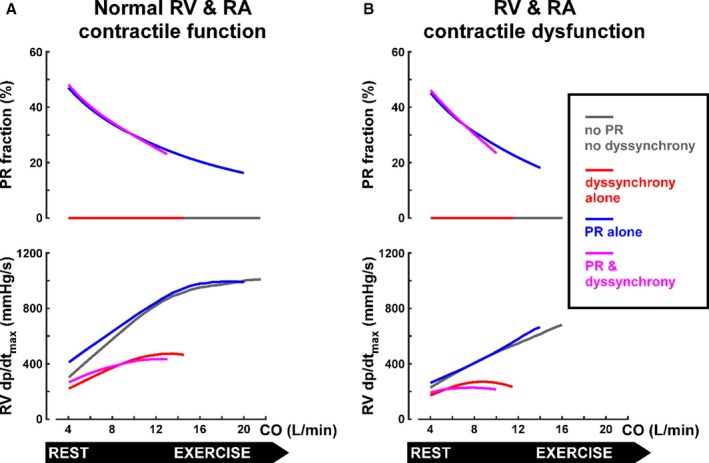
Background The relative impact of right ventricular ( RV ) electromechanical dyssynchrony versus pulmonary regurgitation ( PR ) on exercise capacity and RV function after tetralogy of Fallot repair is unknown. We aimed to delineate the relative effects of these factors on RV function and exercise capacity. Methods and Results We retrospectively analyzed 81 children with tetralogy of Fallot repair using multivariable regression. Predictor parameters were electrocardiographic QRS duration reflecting electromechanical dyssynchrony and PR severity by cardiac magnetic resonance. The outcome parameters were exercise capacity (percentage predicted peak oxygen consumption) and cardiac magnetic resonance ejection fraction (RV ejection fraction). To understand the relative effects of RV dyssynchrony versus PR on exercise capacity and RV function, virtual patient simulations were performed using a closed-loop cardiovascular system model (CircAdapt), covering a wide spectrum of disease severity. Eighty-one patients with tetralogy of Fallot repair (median [interquartile range { IQR} ] age, 14.48 [11.55-15.91] years) were analyzed. All had prolonged QRS duration (median [IQR], 144 [123-152] ms), at least moderate PR (median [IQR], 40% [29%-48%]), reduced exercise capacity (median [IQR], 79% [68%-92%] predicted peak oxygen consumption), and reduced RV ejection fraction (median [IQR], 48% [44%-52%]). Longer QRS duration, more than PR , was associated with lower oxygen consumption and lower RV ejection fraction. In a multivariable regression analysis, oxygen consumption decreased with both increasing QRS duration and PR severity. CircAdapt modeling showed that RV dyssynchrony exerts a stronger limiting effect on exercise capacity and on RV ejection fraction than does PR , regardless of contractile function. Conclusions In both patient data and computer simulations, RV dyssynchrony, more than PR , appears to be associated with reduced exercise capacity and RV systolic dysfunction in patients after TOF repair.
Keywords: computer‐based model; pulmonary regurgitation; right ventricular dysfunction; right ventricular dyssynchrony; tetralogy of Fallot; volume overload.
Figures
Similar articles
-
Factors associated with right ventricular dilatation and dysfunction in patients with chronic pulmonary regurgitation after repair of tetralogy of Fallot: analysis of magnetic resonance imaging data from 218 patients.J Thorac Cardiovasc Surg. 2014 Dec;148(6):2589-95. doi: 10.1016/j.jtcvs.2014.07.051. Epub 2014 Aug 1. J Thorac Cardiovasc Surg. 2014. PMID: 25173118
-
Evolution of Right Ventricular Electromechanical Dyssynchrony During Childhood After Tetralogy of Fallot Repair.Can J Cardiol. 2025 Jun;41(6):1172-1181. doi: 10.1016/j.cjca.2025.02.015. Epub 2025 Feb 11. Can J Cardiol. 2025. PMID: 39947463
-
Mechanisms of right ventricular electromechanical dyssynchrony and mechanical inefficiency in children after repair of tetralogy of fallot.Circ Cardiovasc Imaging. 2014 Jul;7(4):610-8. doi: 10.1161/CIRCIMAGING.113.001483. Epub 2014 May 1. Circ Cardiovasc Imaging. 2014. PMID: 24785673
-
Pulmonary valve replacement after operative repair of tetralogy of Fallot: meta-analysis and meta-regression of 3,118 patients from 48 studies.J Am Coll Cardiol. 2013 Dec 10;62(23):2227-43. doi: 10.1016/j.jacc.2013.04.107. Epub 2013 Sep 28. J Am Coll Cardiol. 2013. PMID: 24080109
-
Timing and type of surgery for severe pulmonary regurgitation after repair of tetralogy of Fallot.Int J Cardiol. 2004 Dec;97 Suppl 1:91-101. doi: 10.1016/j.ijcard.2004.08.013. Int J Cardiol. 2004. PMID: 15590085 Review.
Cited by
-
Outcomes of Transcatheter Pulmonary Valve Replacement and Surgical Pulmonary Valve Replacement: A Cohort Analysis.J Soc Cardiovasc Angiogr Interv. 2022 Aug 2;1(5):100408. doi: 10.1016/j.jscai.2022.100408. eCollection 2022 Sep-Oct. J Soc Cardiovasc Angiogr Interv. 2022. PMID: 39131481 Free PMC article.
-
Management of Fallot's Uncorrected Tetralogy in Adulthood: A Narrative Review.Cureus. 2024 Aug 17;16(8):e67063. doi: 10.7759/cureus.67063. eCollection 2024 Aug. Cureus. 2024. PMID: 39286683 Free PMC article. Review.
-
Right ventricular failure in congenital heart disease.Curr Opin Pediatr. 2019 Oct;31(5):604-610. doi: 10.1097/MOP.0000000000000804. Curr Opin Pediatr. 2019. PMID: 31356354 Free PMC article. Review.
-
Right ventricular dilatation score: a new assessment to right ventricular dilatation in adult patients with repaired tetralogy of Fallot.BMC Cardiovasc Disord. 2023 Sep 14;23(1):458. doi: 10.1186/s12872-023-03487-2. BMC Cardiovasc Disord. 2023. PMID: 37710173 Free PMC article.
-
The Progress and Significance of QRS Duration by Electrocardiography in Hypoplastic Left Heart Syndrome.Pediatr Cardiol. 2020 Jan;41(1):141-148. doi: 10.1007/s00246-019-02237-6. Epub 2019 Nov 13. Pediatr Cardiol. 2020. PMID: 31722042
References
-
- Orwat S, Diller GP, Kempny A, Radke R, Peters B, Kuhne T, Boethig D, Gutberlet M, Dubowy KO, Beerbaum P, Sarikouch S, Baumgartner H; German Competence Network for Congenital Heart Defects Investigators . Myocardial deformation parameters predict outcome in patients with repaired tetralogy of Fallot. Heart. 2016;102:209–215. - PubMed
-
- Valente AM, Gauvreau K, Assenza GE, Babu‐Narayan SV, Schreier J, Gatzoulis MA, Groenink M, Inuzuka R, Kilner PJ, Koyak Z, Landzberg MJ, Mulder B, Powell AJ, Wald R, Geva T. Contemporary predictors of death and sustained ventricular tachycardia in patients with repaired tetralogy of Fallot enrolled in the INDICATOR cohort. Heart. 2014;100:247–253. - PMC - PubMed
-
- Larios G, Friedberg MK. Imaging in repaired tetralogy of Fallot with a focus on recent advances in echocardiography. Curr Opin Cardiol. 2017;32:490–502. - PubMed
-
- Knauth AL, Gauvreau K, Powell AJ, Landzberg MJ, Walsh EP, Lock JE, del Nido PJ, Geva T. Ventricular size and function assessed by cardiac MRI predict major adverse clinical outcomes late after tetralogy of Fallot repair. Heart. 2008;94:211–216. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
