

Helpful ways providers can communicate about persistent medically unexplained physical symptoms
- PMID: 30651073
- PMCID: PMC6334465
- DOI: 10.1186/s12875-018-0881-8
Helpful ways providers can communicate about persistent medically unexplained physical symptoms
Abstract
Background: Communication between patients and providers about persistent "medically unexplained" physical symptoms (MUS) is characterized by discordance. While the difficulties are well documented, few studies have examined effective communication. We sought to determine what veterans with Gulf War Illness (GWI) perceive as the most helpful communication from their providers. Veterans with GWI, a type of MUS, have historically had complex relationships with medical providers. Determining effective communication for patients with particularly complex relationships may help identify the most critical communication elements for all patients with MUS.
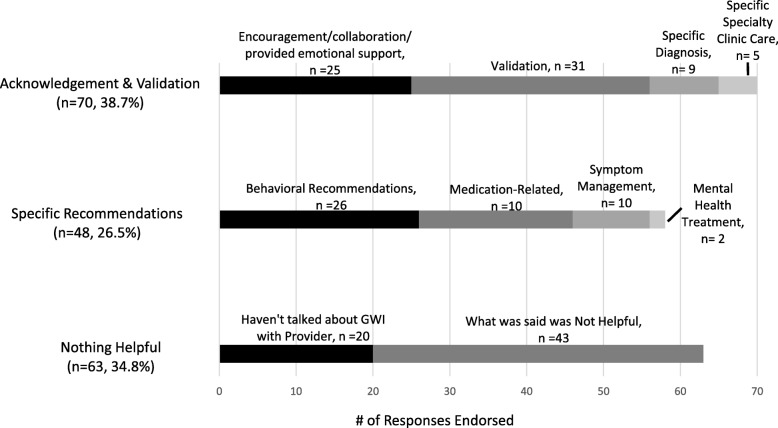
Methods: Two hundred and-ten veterans with GWI were asked, in a written questionnaire, what was the most useful thing a medical provider had told them about their GWI. Responses were coded into three categories with 10 codes.
Results: The most prevalent helpful communication reported by patients was when the provider offered acknowledgement and validation (N = 70). Specific recommendations for managing GWI or its symptoms (N = 48) were also commonly reported to be helpful. In contrast, about a third of the responses indicated that nothing about the communication was helpful (N = 63). There were not differences in severity of symptoms, disability or healthcare utilization between patients who found acknowledgement and validation, specific recommendations or nothing helpful.
Conclusions: Previous research has documented the discord between patients and providers regarding MUS. This study suggests that most patients are able to identify something helpful a provider has said, particularly acknowledgement and validation and specific treatment recommendations. The findings also highlight missed communication opportunities with a third of patients not finding anything helpful.
Keywords: Gulf war illness; Medically unexplained symptoms; Patient provider communication; Patient provider relationship; Qualitative; Veteran.
Conflict of interest statement
Ethics approval and consent to participate
All participants provided written consent to be part of this study and to have the data published. The study was reviewed by the Veterans Affairs New Jersey Healthcare System Institutional Review Board, Canandaigua VA Medical Center Institutional Review Board, and Edith Nourse Rogers Memorial VA Hospital Institutional Review Board. I confirm all patient/personal identifiers have been removed or disguised so the patient/person(s) described are not identifiable and cannot be identified through the details of the story.
Consent for publication
Not Applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
