

Late effects of pediatric hematopoietic stem cell transplantation on left ventricular function, aortic stiffness and myocardial tissue characteristics
- PMID: 30651110
- PMCID: PMC6335808
- DOI: 10.1186/s12968-018-0513-4
Late effects of pediatric hematopoietic stem cell transplantation on left ventricular function, aortic stiffness and myocardial tissue characteristics
Abstract
Background: Pediatric hematopoietic stem cell transplantation (HSCT) recipients are at increased risk of cardiovascular disease later in life. As HSCT survival has significantly improved, with a growing number of HSCT indications, tailored screening strategies for HSCT-related late effects are warranted. Little is known regarding the value of cardiovascular magnetic resonance (CMR) for early identification of high-risk patients after HSCT, before symptomatic cardiovascular disease manifests. This study aimed to assess CMR-derived left ventricular (LV) systolic and diastolic function, aortic stiffness and myocardial tissue characteristics in young adults who received HSCT during childhood.
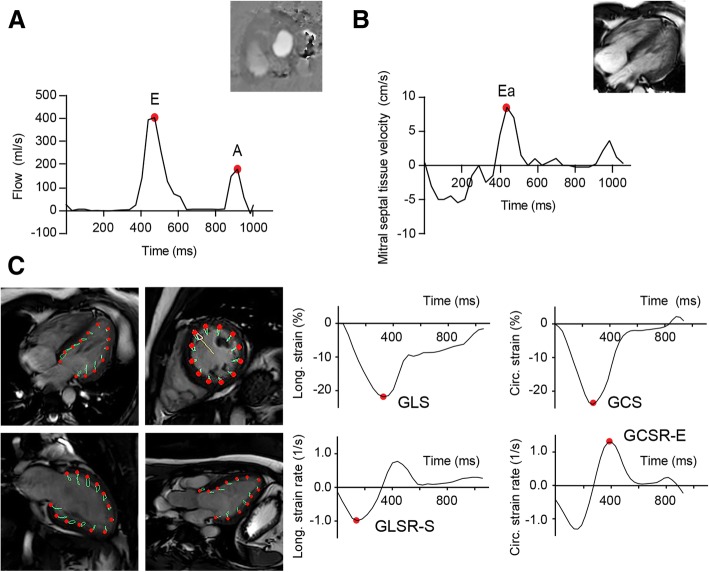
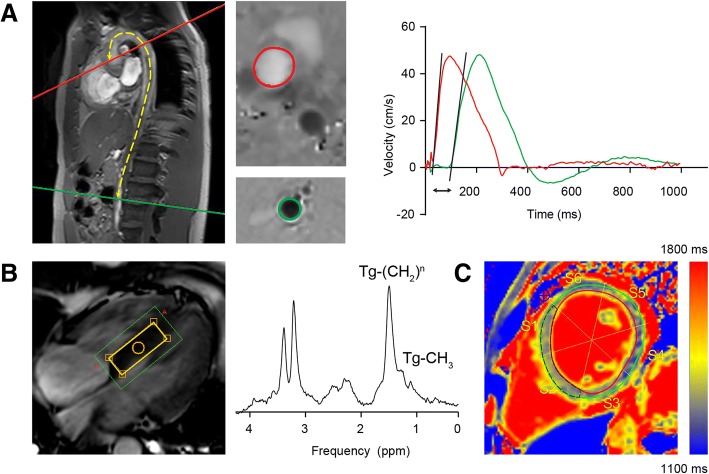
Methods: Sixteen patients (22.1 ± 1.5 years) treated with HSCT during childhood and 16 healthy controls (22.1 ± 1.8 years) underwent 3 T CMR. LV systolic and diastolic function were measured as LV ejection fraction (LVEF), the ratio of transmitral early and late peak filling rate (E/A), the estimated LV filling pressure (E/Ea) and global longitudinal and circumferential systolic strain and diastolic strain rates, using balanced steady-state free precession cine CMR and 2D velocity-encoded CMR over the mitral valve. Aortic stiffness, myocardial fibrosis and steatosis were assessed with 2D velocity-encoded CMR, native T1 mapping and proton CMR spectroscopy (1H-CMRS), respectively.
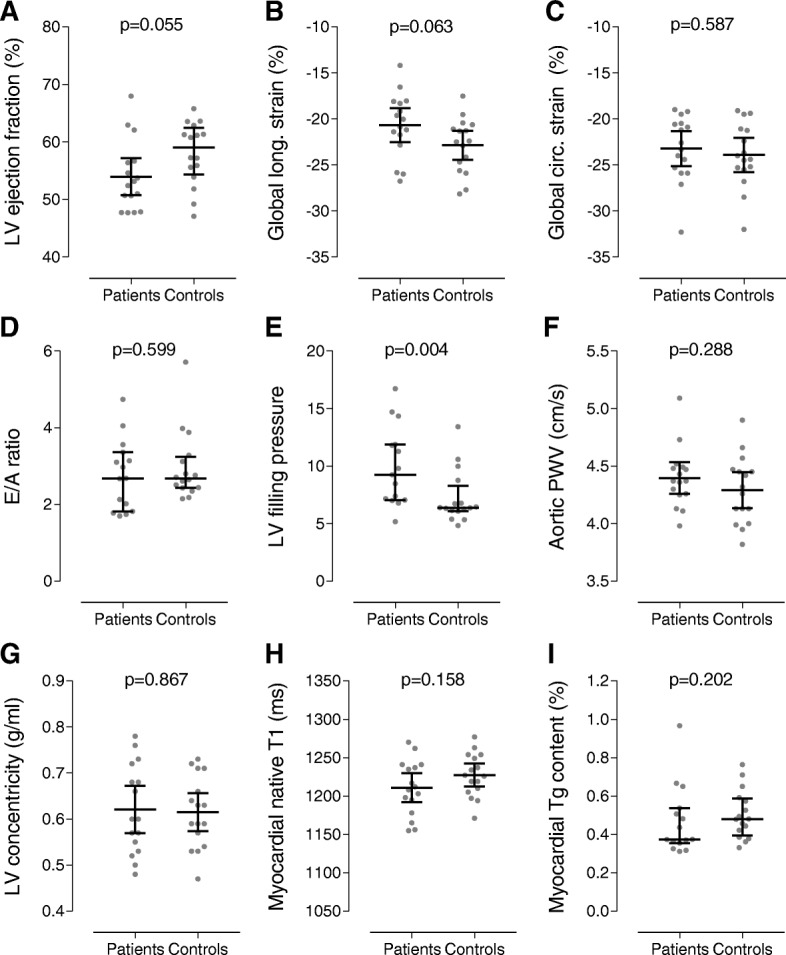
Results: In the patient compared to the control group, E/Ea (9.92 ± 3.42 vs. 7.24 ± 2.29, P = 0.004) was higher, LVEF (54 ± 6% vs. 58 ± 5%, P = 0.055) and global longitudinal strain (GLS) ( -20.7 ± 3.5% vs. -22.9 ± 3.0%, P = 0.063) tended to be lower, while aortic pulse wave velocity (4.40 ± 0.26 vs. 4.29 ± 0.29 m/s, P = 0.29), native T1 (1211 ± 36 vs. 1227 ± 28 ms, P = 0.16) and myocardial triglyceride content (0.47 ± 0.18 vs. 0.50 ± 0.13%, P = 0.202) were comparable. There were no differences between patients and controls in E/A (2.76 ± 0.92 vs. 2.97 ± 0.91, P = 0.60) and diastolic strain rates.
Conclusion: In young adults who received HSCT during childhood, LV diastolic function was decreased (higher estimated LV filling pressure) and LV systolic function (LVEF and GLS) tended to be reduced as compared to healthy controls, whereas no concomitant differences were found in aortic stiffness and myocardial tissue characteristics. When using CMR, assessment of LV diastolic function in particular is important for early detection of patients at risk of HSCT-related cardiovascular disease, which may warrant closer surveillance.
Keywords: Aortic stiffness; Cardiovascular magnetic resonance; Diffuse fibrosis; Hematopoietic stem cell transplantation; Myocardial steatosis; Pediatric; Systolic and diastolic function; T1 mapping.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the local institutional review board (Leiden University Medical Center, the Netherlands) and complies with the Declaration of Helsinki. All participants provided written informed consent prior to enrolment into the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Early detection of subclinical ventricular deterioration in aortic stenosis with cardiovascular magnetic resonance and echocardiography.J Cardiovasc Magn Reson. 2013 Aug 28;15(1):72. doi: 10.1186/1532-429X-15-72. J Cardiovasc Magn Reson. 2013. PMID: 23984681 Free PMC article.
-
Cardiovascular magnetic resonance feature tracking for characterization of patients with heart failure with preserved ejection fraction: correlation of global longitudinal strain with invasive diastolic functional indices.J Cardiovasc Magn Reson. 2020 Jun 4;22(1):42. doi: 10.1186/s12968-020-00636-w. J Cardiovasc Magn Reson. 2020. PMID: 32498688 Free PMC article.
-
Phenotyping diabetic cardiomyopathy in Europeans and South Asians.Cardiovasc Diabetol. 2019 Oct 11;18(1):133. doi: 10.1186/s12933-019-0940-z. Cardiovasc Diabetol. 2019. PMID: 31604432 Free PMC article.
-
Cardiovascular magnetic resonance in an adult human population: serial observations from the multi-ethnic study of atherosclerosis.J Cardiovasc Magn Reson. 2017 Jul 18;19(1):52. doi: 10.1186/s12968-017-0367-1. J Cardiovasc Magn Reson. 2017. PMID: 28720123 Free PMC article. Review.
-
Evaluation of left ventricular torsion by cardiovascular magnetic resonance.J Cardiovasc Magn Reson. 2012 Jul 24;14(1):49. doi: 10.1186/1532-429X-14-49. J Cardiovasc Magn Reson. 2012. PMID: 22827856 Free PMC article. Review.
Cited by
-
Rapid cardiovascular aging following allogeneic hematopoietic cell transplantation for hematological malignancy.Front Cardiovasc Med. 2022 Dec 15;9:926064. doi: 10.3389/fcvm.2022.926064. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36588564 Free PMC article.
-
T1 Mapping in Cardiovascular Magnetic Resonance-A Marker of Diffuse Myocardial Fibrosis in Patients Undergoing Hematopoietic Stem Cell Transplantation.J Pers Med. 2024 Apr 13;14(4):412. doi: 10.3390/jpm14040412. J Pers Med. 2024. PMID: 38673039 Free PMC article.
-
Cardiorespiratory fitness and physical performance after childhood hematopoietic stem cell transplantation: a systematic review and meta-analysis.Bone Marrow Transplant. 2021 Sep;56(9):2063-2078. doi: 10.1038/s41409-021-01370-2. Epub 2021 Jun 21. Bone Marrow Transplant. 2021. PMID: 34155356
References
-
- Uderzo C, Pillon M, Corti P, Tridello G, Tana F, Zintl F, et al. Impact of cumulative anthracycline dose, preparative regimen and chronic graft-versus-host disease on pulmonary and cardiac function in children 5 years after allogeneic hematopoietic stem cell transplantation: a prospective evaluation on behalf of the EBMT pediatric diseases and late effects working parties. Bone Marrow Transplant. 2007;39(11):667–675. doi: 10.1038/sj.bmt.1705652. - DOI - PubMed
-
- Lipshultz SE, Adams MJ, Colan SD, Constine LS, Herman EH, Hsu DT, et al. Long-term cardiovascular toxicity in children, adolescents, and young adults who receive cancer therapy: pathophysiology, course, monitoring, management, prevention, and research directions: a scientific statement from the American Heart Association. Circulation. 2013;128(17):1927–1995. doi: 10.1161/CIR.0b013e3182a88099. - DOI - PubMed
-
- Niederwieser D, Baldomero H, Szer J, Gratwohl M, Aljurf M, Atsuta Y, et al. Hematopoietic stem cell transplantation activity worldwide in 2012 and a SWOT analysis of the worldwide network for blood and marrow transplantation group including the global survey. Bone Marrow Transplant. 2016;51(6):778–785. doi: 10.1038/bmt.2016.18. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
