

Common conditions associated with hereditary haemochromatosis genetic variants: cohort study in UK Biobank
- PMID: 30651232
- PMCID: PMC6334179
- DOI: 10.1136/bmj.k5222
Common conditions associated with hereditary haemochromatosis genetic variants: cohort study in UK Biobank
Erratum in
-
Common conditions associated with hereditary haemochromatosis genetic variants: cohort study in UK Biobank.BMJ. 2019 Oct 23;367:l6157. doi: 10.1136/bmj.l6157. BMJ. 2019. PMID: 31645331 Free PMC article. No abstract available.
Abstract
Objective: To compare prevalent and incident morbidity and mortality between those with the HFE p.C282Y genetic variant (responsible for most hereditary haemochromatosis type 1) and those with no p.C282Y mutations, in a large UK community sample of European descent.
Design: Cohort study.
Setting: 22 centres across England, Scotland, and Wales in UK Biobank (2006-10).
Participants: 451 243 volunteers of European descent aged 40 to 70 years, with a mean follow-up of seven years (maximum 9.4 years) through hospital inpatient diagnoses and death certification.
Main outcome measure: Odds ratios and Cox hazard ratios of disease rates between participants with and without the haemochromatosis mutations, adjusted for age, genotyping array type, and genetic principal components. The sexes were analysed separately as morbidity due to iron excess occurs later in women.
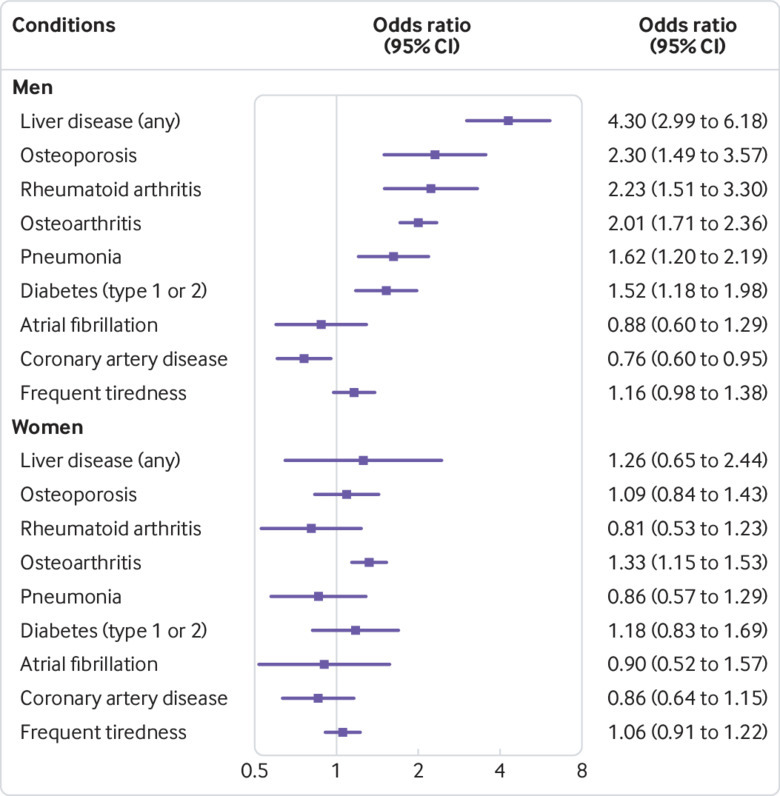
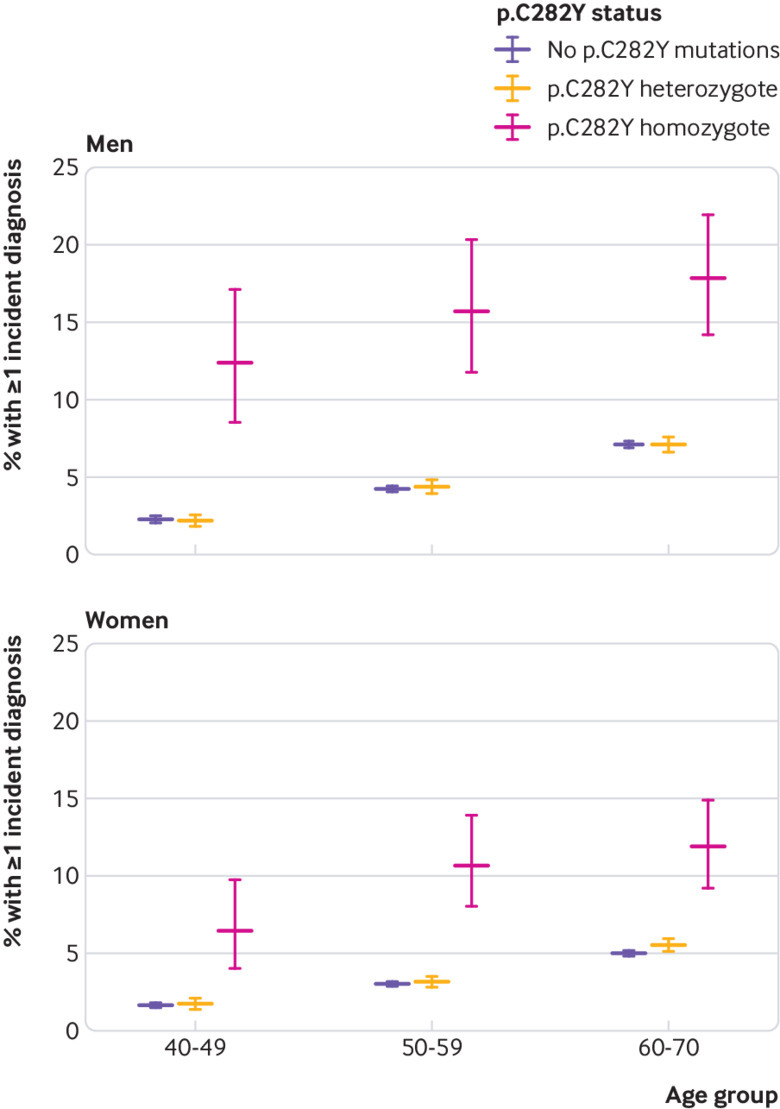
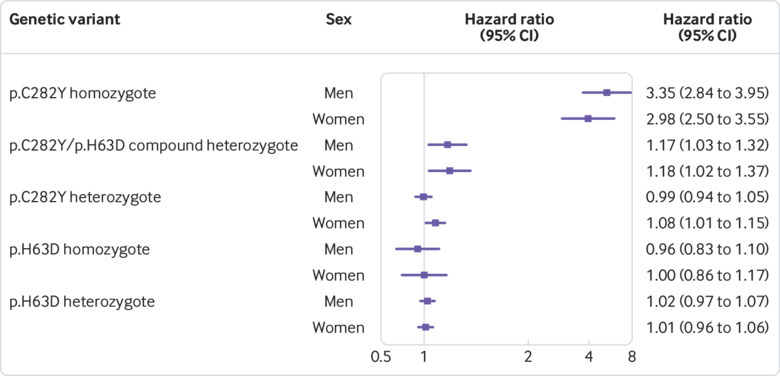
Results: Of 2890 participants homozygous for p.C282Y (0.6%, or 1 in 156), haemochromatosis was diagnosed in 21.7% (95% confidence interval 19.5% to 24.1%, 281/1294) of men and 9.8% (8.4% to 11.2%, 156/1596) of women by end of follow-up. p.C282Y homozygous men aged 40 to 70 had a higher prevalence of diagnosed haemochromatosis (odds ratio 411.1, 95% confidence interval 299.0 to 565.3, P<0.001), liver disease (4.30, 2.97 to 6.18, P<0.001), rheumatoid arthritis (2.23, 1.51 to 3.31, P<0.001), osteoarthritis (2.01, 1.71 to 2.36, P<0.001), and diabetes mellitus (1.53, 1.16 to 1.98, P=0.002), versus no p.C282Y mutations (n=175 539). During the seven year follow-up, 15.7% of homozygous men developed at least one incident associated condition versus 5.0% (P<0.001) with no p.C282Y mutations (women 10.1% v 3.4%, P<0.001). Haemochromatosis diagnoses were more common in p.C282Y/p.H63D heterozygotes, but excess morbidity was modest.
Conclusions: In a large community sample, HFE p.C282Y homozygosity was associated with substantial prevalent and incident clinically diagnosed morbidity in both men and women. As p.C282Y associated iron overload is preventable and treatable if intervention starts early, these findings justify re-examination of options for expanded early case ascertainment and screening.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form (at www.icmje.org/coi_disclosure.pdf) and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials