

Clinical-grade stem cell-derived retinal pigment epithelium patch rescues retinal degeneration in rodents and pigs
- PMID: 30651323
- PMCID: PMC8784963
- DOI: 10.1126/scitranslmed.aat5580
Clinical-grade stem cell-derived retinal pigment epithelium patch rescues retinal degeneration in rodents and pigs
Erratum in
-
Erratum for the Research Article: "Clinical-grade stem cell-derived retinal pigment epithelium patch rescues retinal degeneration in rodents and pigs" by R. Sharma, V. Khristov, A. Rising, B. S. Jha, R. Dejene, N. Hotaling, Y. Li, J. Stoddard, C. Stankewicz, Q. Wan, C. Zhang, M. M. Campos, K. J. Miyagishima, D. McGaughey, R. Villasmil, M. Mattapallil, B. Stanzel, H. Qian, W. Wong, L. Chase, S. Charles, T. McGill, S. Miller, A. Maminishkis, J. Amaral, K. Bharti.Sci Transl Med. 2019 Feb 6;11(478):eaaw7624. doi: 10.1126/scitranslmed.aaw7624. Sci Transl Med. 2019. PMID: 30728289 No abstract available.
Abstract
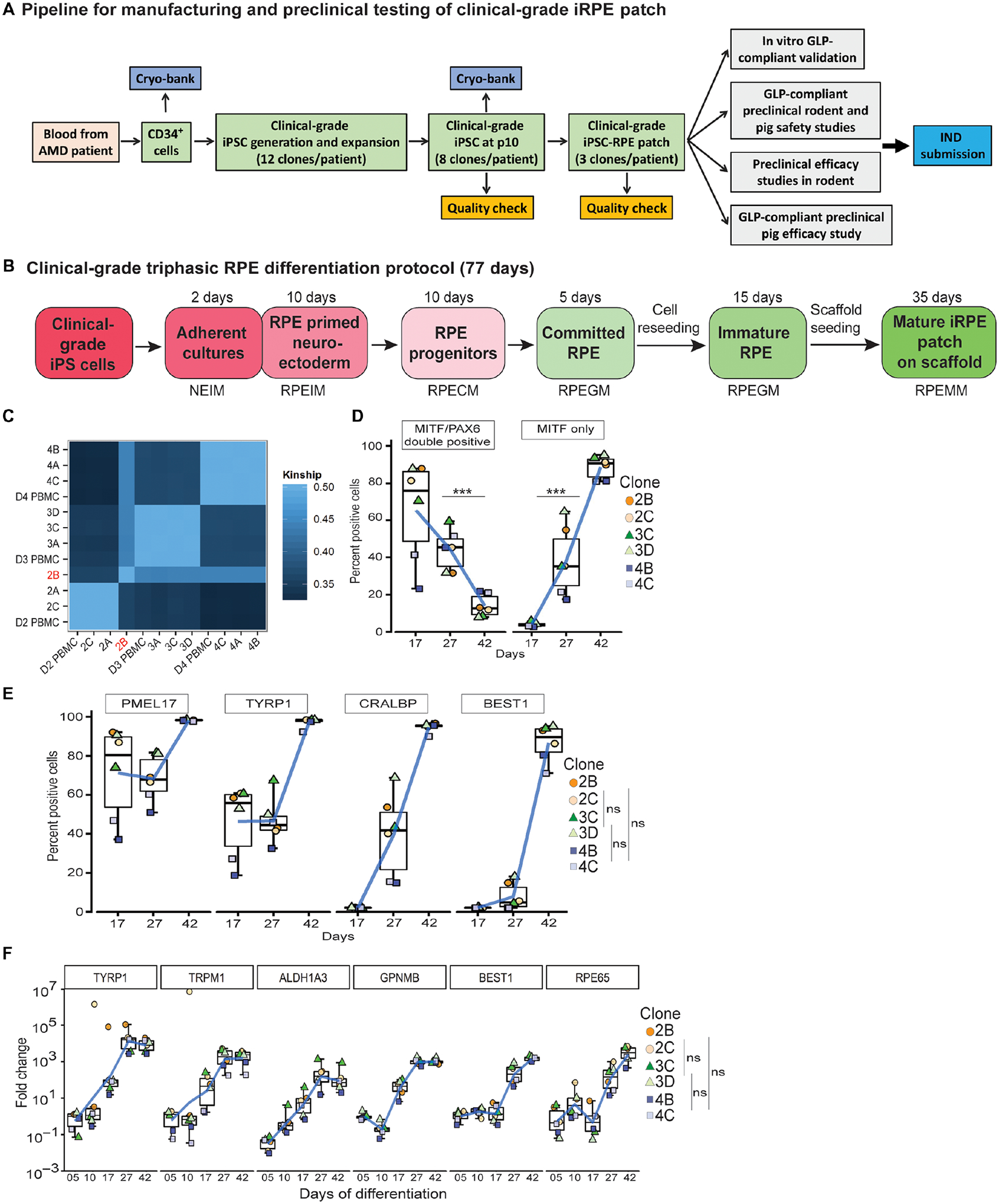
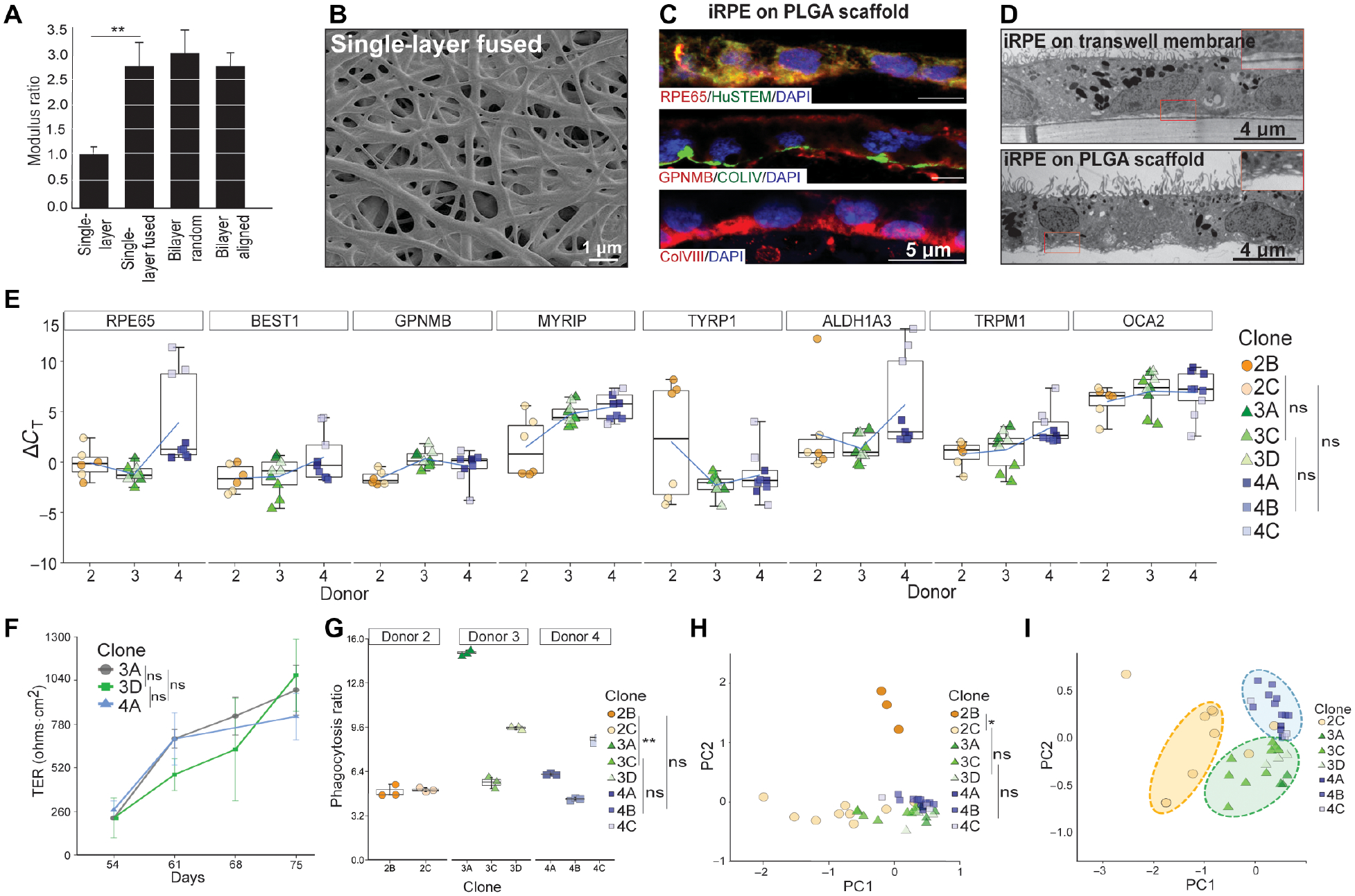
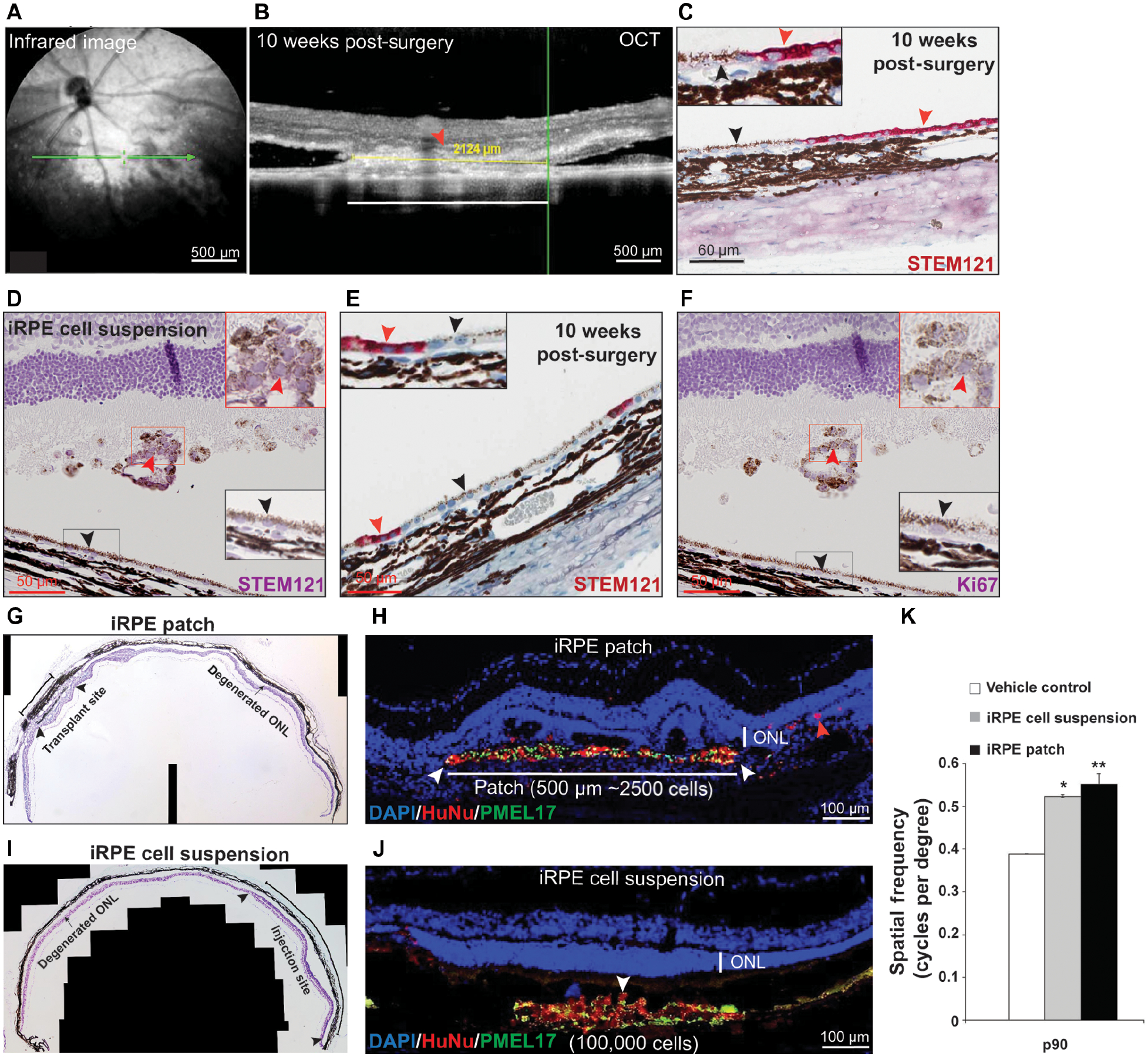
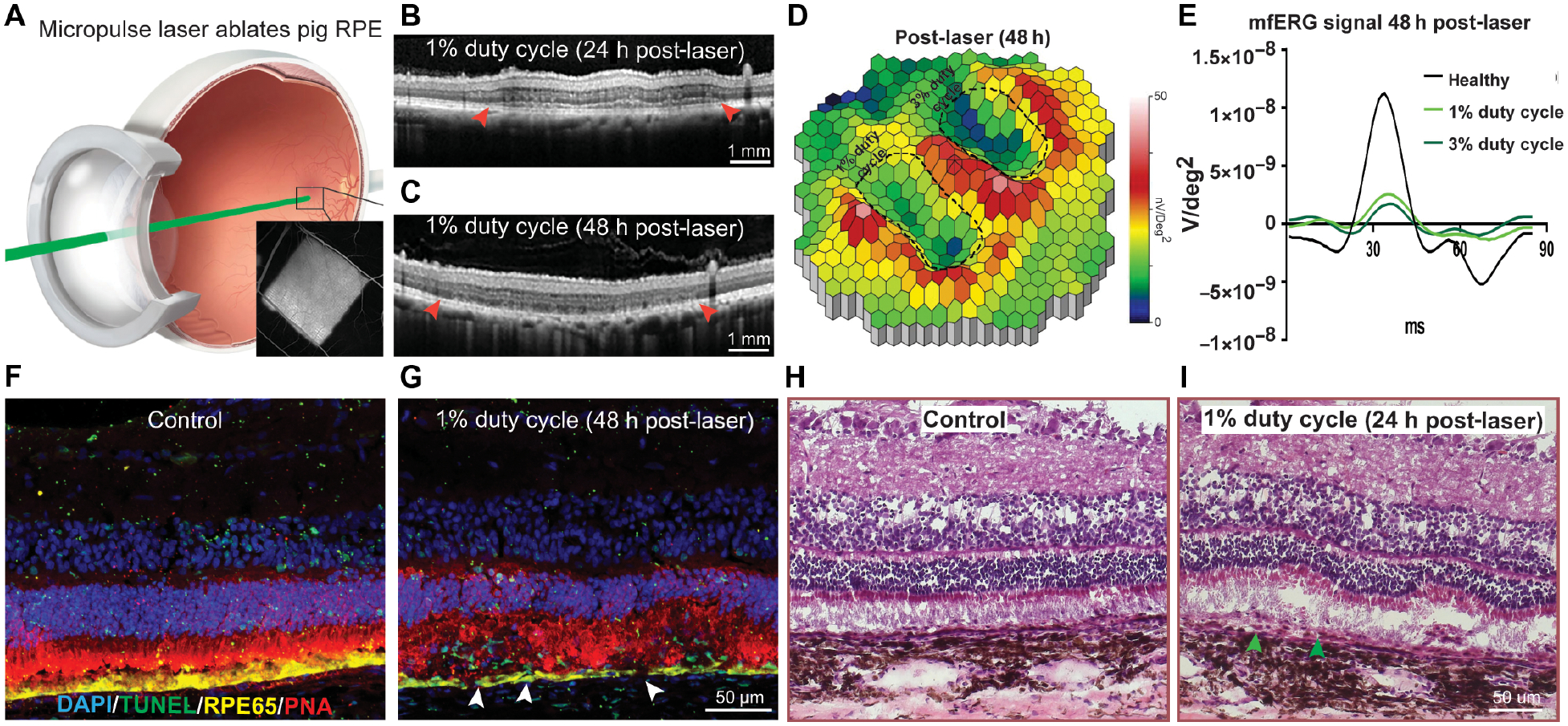
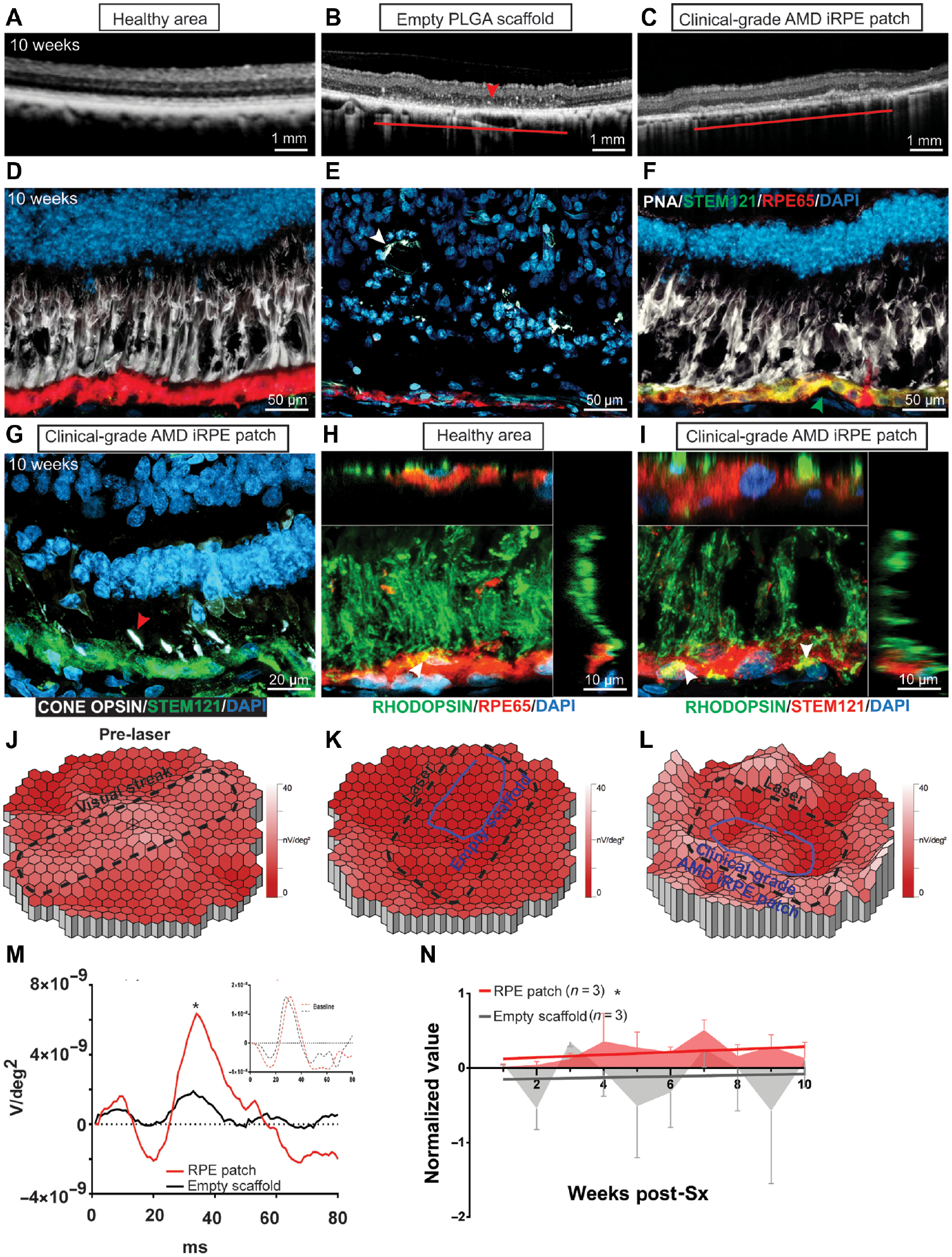
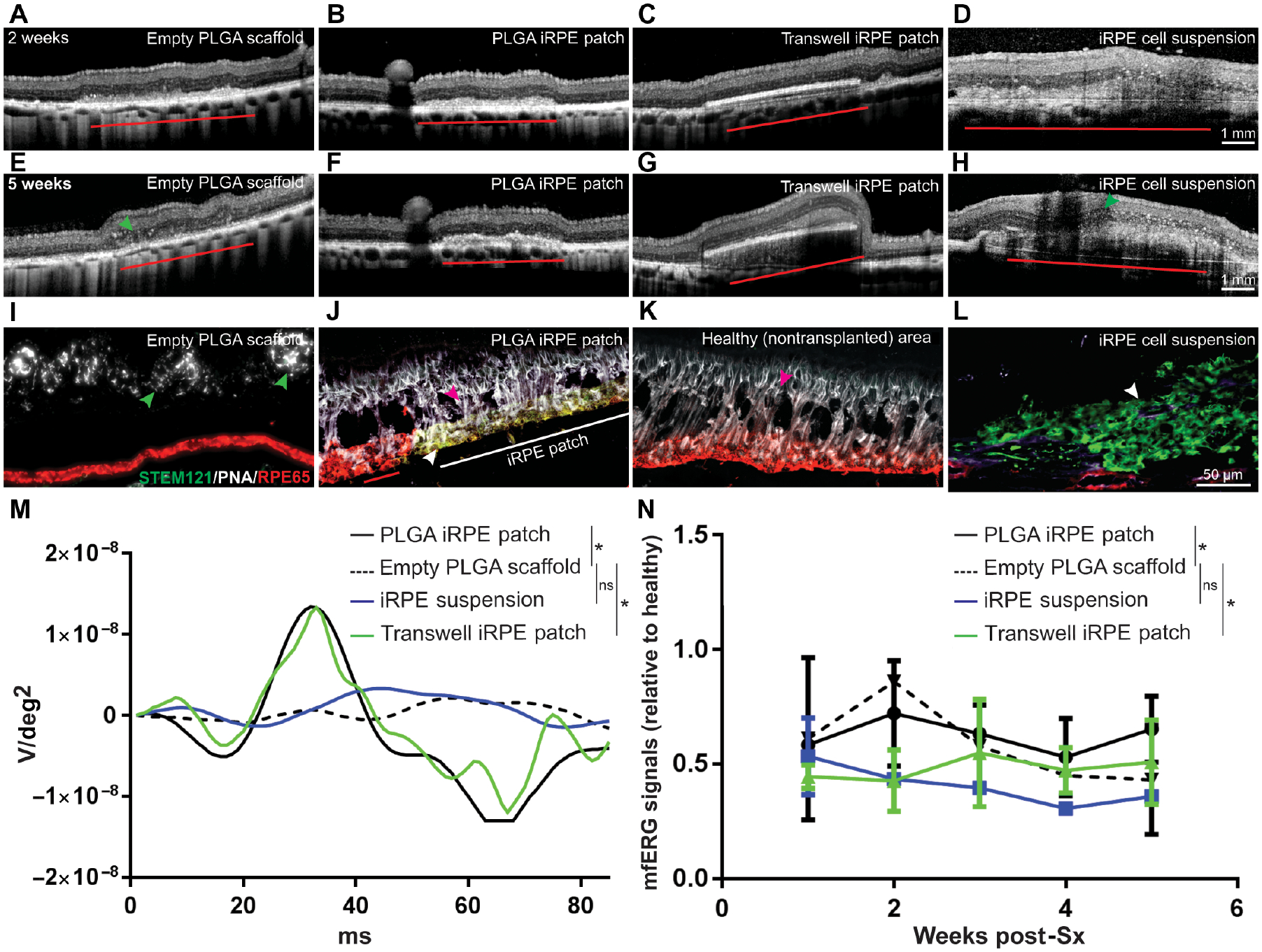
Considerable progress has been made in testing stem cell-derived retinal pigment epithelium (RPE) as a potential therapy for age-related macular degeneration (AMD). However, the recent reports of oncogenic mutations in induced pluripotent stem cells (iPSCs) underlie the need for robust manufacturing and functional validation of clinical-grade iPSC-derived RPE before transplantation. Here, we developed oncogenic mutation-free clinical-grade iPSCs from three AMD patients and differentiated them into clinical-grade iPSC-RPE patches on biodegradable scaffolds. Functional validation of clinical-grade iPSC-RPE patches revealed specific features that distinguished transplantable from nontransplantable patches. Compared to RPE cells in suspension, our biodegradable scaffold approach improved integration and functionality of RPE patches in rats and in a porcine laser-induced RPE injury model that mimics AMD-like eye conditions. Our results suggest that the in vitro and in vivo preclinical functional validation of iPSC-RPE patches developed here might ultimately be useful for evaluation and optimization of autologous iPSC-based therapies.
Copyright © 2019 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Conflict of interest statement
Figures
References
-
- Joussen AM et al. , Autologous translocation of the choroid and retinal pigment epithelium in patients with geographic atrophy. Ophthalmology 114, 551–560 (2007). - PubMed
-
- van Zeeburg EJ, Maaijwee KJ, Missotten TO, Heimann H, van Meurs JC, A free retinal pigment epithelium-choroid graft in patients with exudative age-related macular degeneration: results up to 7 years. Am J Ophthalmol 153, 120–127.e122 (2012). - PubMed
-
- Schwartz SD et al. , Embryonic stem cell trials for macular degeneration: a preliminary report. Lancet 379, 713–720 (2012). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
