

Long-term graft patency after coronary artery bypass grafting: Effects of surgical technique
- PMID: 30651804
- PMCID: PMC6307371
- DOI: 10.3892/etm.2018.6929
Long-term graft patency after coronary artery bypass grafting: Effects of surgical technique
Abstract
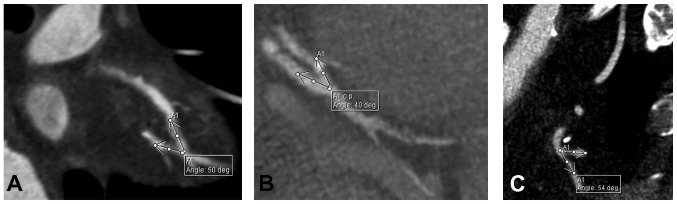
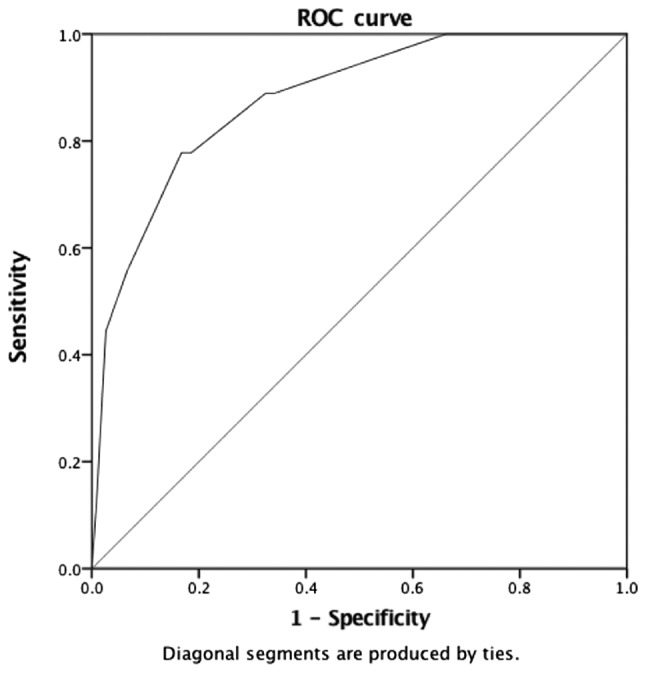
The aim of the current study was to identify surgical factors associated with long-term patency of grafts used in coronary artery bypass grafting (CABG). The present study analyzed data from 127 patients who underwent CABG at our institute between 2000 and 2006 and presented for ambulatory examination and coronary computed tomography angiography evaluation of graft patency in 2016 (139.78±36.64 months post-CABG). The 127 patients received 340 grafts (2.68 grafts/patient) and 399 distal anastomoses (3.14 anastomoses/patient), 220 (55.14%) with arterial grafts and 179 (44.86%) with saphenous vein grafts. Graft patency varied according to coronary territory, proximal anastomosis type (in situ graft, composite graft, graft anastomosed to the ascending aorta), Y anastomosis angle (47.21° for patent arterial grafts vs. 56° for occluded), and distal anastomosis angle (in sequential anastomoses irrespective to graft type, 48.60° for patent side-to-side anastomosis vs. 53.97° for occluded, 65.12° for patent end-to-side anastomosis vs. 90.80° for occluded; in single end-to-side anastomosis of arterial grafts, 39.46° for patent and 44.94° for occluded). A single end-to-side anastomosis angle 60° or greater was associated with a 5.149 occlusion odds ratio (OR) (P<0.001) for arterial grafts. Venous grafts were not sensitive to single end-to-side anastomosis angle. In conclusion, a small anastomosis angle for proximal Y and distal anastomoses is associated with a higher long-term patency of the free graft. Radial artery grafts registered higher patency rates when anastomosed to the ascending aorta compared with composite grafting with the left internal thoracic artery, whereas in situ right internal thoracic artery (RITA) anastomosed to the right coronary territory is associated with a lower patency rate compared with free RITA used to revascularise the anterolateral or circumflex territory in composite grafting.
Keywords: anastomosis angle; anastomosis type; composite grafting; coronary artery bypass grafting; long-term patency.
Figures

Similar articles
-
Long-term graft patency after coronary artery bypass grafting: Effects of morphological and pathophysiological factors.Anatol J Cardiol. 2018 Nov;20(5):275-282. doi: 10.14744/AnatolJCardiol.2018.51447. Anatol J Cardiol. 2018. PMID: 30391966 Free PMC article.
-
V-composite grafting using the right internal thoracic artery grafts anastomosed to aorto-coronary bypass grafts.Eur J Cardiothorac Surg. 2015 Nov;48(5):753-7. doi: 10.1093/ejcts/ezu525. Epub 2015 Jan 18. Eur J Cardiothorac Surg. 2015. PMID: 25602057
-
Rationale for off-pump coronary revascularization to small branches--angiographic study of 1,283 anastomoses in 408 patients.Ann Thorac Surg. 2004 May;77(5):1530-4. doi: 10.1016/j.athoracsur.2003.10.043. Ann Thorac Surg. 2004. PMID: 15111137
-
Composite arterial grafting.Expert Rev Cardiovasc Ther. 2006 Jul;4(4):523-33. doi: 10.1586/14779072.4.4.523. Expert Rev Cardiovasc Ther. 2006. PMID: 16918271 Review.
-
Saphenous vein graft vs. radial artery graft searching for the best second coronary artery bypass graft.J Saudi Heart Assoc. 2013 Oct;25(4):247-54. doi: 10.1016/j.jsha.2013.06.001. J Saudi Heart Assoc. 2013. PMID: 24198449 Free PMC article. Review.
Cited by
-
Improvement of the outcome of the saphenous vein graft when connected to the internal thoracic artery.Front Cardiovasc Med. 2024 Oct 18;11:1478166. doi: 10.3389/fcvm.2024.1478166. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39494236 Free PMC article.
-
A mathematical model to evaluate hemodynamic effects of the graft anastomosis in coronary surgery.Kardiochir Torakochirurgia Pol. 2019 Jul;16(2):106-108. doi: 10.5114/kitp.2019.86366. Epub 2019 Jun 28. Kardiochir Torakochirurgia Pol. 2019. PMID: 31410101 Free PMC article.
-
Sex-specific disparities in patients undergoing isolated CABG.Am Heart J Plus. 2023 Oct 19;35:100334. doi: 10.1016/j.ahjo.2023.100334. eCollection 2023 Nov. Am Heart J Plus. 2023. PMID: 38511179 Free PMC article.
-
Revealing the Process of Vein Graft Failure: A Panoramic Review from Etiology Analysis to Mechanism Explanation and Treatment Strategy.Cardiovasc Drugs Ther. 2025 May 29. doi: 10.1007/s10557-025-07711-3. Online ahead of print. Cardiovasc Drugs Ther. 2025. PMID: 40439962 Review.
-
Anatomy of the septal perforating arteries of the heart.Anat Cell Biol. 2019 Sep;52(3):236-241. doi: 10.5115/acb.18.175. Epub 2019 Aug 26. Anat Cell Biol. 2019. PMID: 31598351 Free PMC article. Review.
References
-
- http://ec.europa.eu/eurostat/statistics-explained/index.php/Cardiovascul.... [Aug 31;2017 ];Eurostat-Cardiovascular diseases statistics.
-
- http://ec.europa.eu/eurostat/statistics-explained/index.php/Surgical_ope.... [Aug 31;2017 ];Eurostat-Surgical operations and procedures statistics.
-
- Authors/Task Force members, corp-author. Windecker S, Kolh P, Alfonso F, Collet JP, Cremer J, Falk V, Filippatos G, Hamm C, Head SJ, et al. 2014 ESC/EACTS guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI) Eur Heart J. 2014;35:2541–2619. doi: 10.1093/eurheartj/ehu278. - DOI - PubMed
-
- Coronary Revascularization Writing Group, corp-author. Patel FR, Dehmer GJ, Hirshfeld JW, Smith PK, Spertus JA, Technical Panel. Masoudi FA, Dehmer GJ, Patel MR, et al. ACCF/SCAI/STS/AATS/AHA/ASNC/HFSA/SCCT 2012 appropriate use criteria for coronary revascularization focused update: A report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, Society for Cardiovascular Angiography and Interventions, Society of Thoracic Surgeons, American Association for Thoracic Surgery, American Heart Association, American Society of Nuclear Cardiology, and the Society of Cardiovascular Computed Tomography. J Thorac Cardiovasc Surg. 2012;143:780–803. doi: 10.1016/j.jtcvs.2012.01.061. - DOI - PubMed
LinkOut - more resources
Full Text Sources